Related Research Articles

Hyperthyroidism is the condition that occurs due to excessive production of thyroid hormones by the thyroid gland. Thyrotoxicosis is the condition that occurs due to excessive thyroid hormone of any cause and therefore includes hyperthyroidism. Some, however, use the terms interchangeably. Signs and symptoms vary between people and may include irritability, muscle weakness, sleeping problems, a fast heartbeat, heat intolerance, diarrhea, enlargement of the thyroid, hand tremor, and weight loss. Symptoms are typically less severe in the elderly and during pregnancy. An uncommon but life-threatening complication is thyroid storm in which an event such as an infection results in worsening symptoms such as confusion and a high temperature; this often results in death. The opposite is hypothyroidism, when the thyroid gland does not make enough thyroid hormone.

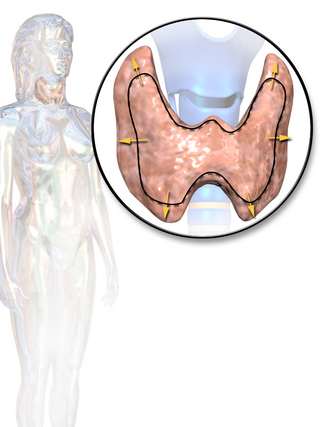
The thyroid, or thyroid gland, is an endocrine gland in vertebrates. In humans, it is in the neck and consists of two connected lobes. The lower two thirds of the lobes are connected by a thin band of tissue called the isthmus (PL: isthmi). The thyroid gland is a butterfly-shaped gland located in the neck below the Adam's apple. Microscopically, the functional unit of the thyroid gland is the spherical thyroid follicle, lined with follicular cells (thyrocytes), and occasional parafollicular cells that surround a lumen containing colloid. The thyroid gland secretes three hormones: the two thyroid hormones – triiodothyronine (T3) and thyroxine (T4) – and a peptide hormone, calcitonin. The thyroid hormones influence the metabolic rate and protein synthesis and growth and development in children. Calcitonin plays a role in calcium homeostasis. Secretion of the two thyroid hormones is regulated by thyroid-stimulating hormone (TSH), which is secreted from the anterior pituitary gland. TSH is regulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus.

Graves' disease, also known as toxic diffuse goiter, is an autoimmune disease that affects the thyroid. It frequently results in and is the most common cause of hyperthyroidism. It also often results in an enlarged thyroid. Signs and symptoms of hyperthyroidism may include irritability, muscle weakness, sleeping problems, a fast heartbeat, poor tolerance of heat, diarrhea and unintentional weight loss. Other symptoms may include thickening of the skin on the shins, known as pretibial myxedema, and eye bulging, a condition caused by Graves' ophthalmopathy. About 25 to 30% of people with the condition develop eye problems.
Hypothyroidism is a disorder of the endocrine system in which the thyroid gland does not produce enough thyroid hormone. It can cause a number of symptoms, such as poor ability to tolerate cold, a feeling of tiredness, constipation, slow heart rate, depression, and weight gain. Occasionally there may be swelling of the front part of the neck due to goitre. Untreated cases of hypothyroidism during pregnancy can lead to delays in growth and intellectual development in the baby or congenital iodine deficiency syndrome.

Congenital hypothyroidism (CH) is thyroid hormone deficiency present at birth. If untreated for several months after birth, severe congenital hypothyroidism can lead to growth failure and permanent intellectual disability. Infants born with congenital hypothyroidism may show no effects, or may display mild effects that often go unrecognized as a problem. Significant deficiency may cause excessive sleeping, reduced interest in nursing, poor muscle tone, low or hoarse cry, infrequent bowel movements, significant jaundice, and low body temperature.
Thyroid-stimulating hormone (also known as thyrotropin, thyrotropic hormone, or abbreviated TSH) is a pituitary hormone that stimulates the thyroid gland to produce thyroxine (T4), and then triiodothyronine (T3) which stimulates the metabolism of almost every tissue in the body. It is a glycoprotein hormone produced by thyrotrope cells in the anterior pituitary gland, which regulates the endocrine function of the thyroid.

Myxedema is a term used synonymously with severe hypothyroidism. However, the term is also used to describe a dermatological change that can occur in hypothyroidism and (rare) paradoxical cases of hyperthyroidism. In this latter sense, myxedema refers to deposition of mucopolysaccharides in the dermis, which results in swelling of the affected area. One manifestation of myxedema occurring in the lower limb is pretibial myxedema, a hallmark of Graves disease, an autoimmune form of hyperthyroidism. Myxedema can also occur in Hashimoto thyroiditis and other long-standing forms of hypothyroidism.

Hashimoto's thyroiditis, also known as chronic lymphocytic thyroiditis and Hashimoto's disease, is an autoimmune disease in which the thyroid gland is gradually destroyed. Early on, symptoms may not be noticed. Over time, the thyroid may enlarge, forming a painless goiter. Some people eventually develop hypothyroidism with accompanying weight gain, fatigue, constipation, depression, hair loss, and general pains. After many years the thyroid typically shrinks in size. Potential complications include thyroid lymphoma. Furthermore, because it is common for untreated patients of Hashimoto's to develop hypothyroidism, further complications can include, but are not limited to, high cholesterol, heart disease, heart failure, high blood pressure, myxedema, and potential pregnancy problems.

Levothyroxine, also known as L-thyroxine, is a synthetic form of the thyroid hormone thyroxine (T4). It is used to treat thyroid hormone deficiency (hypothyroidism), including a severe form known as myxedema coma. It may also be used to treat and prevent certain types of thyroid tumors. It is not indicated for weight loss. Levothyroxine is taken orally (by mouth) or given by intravenous injection. Levothyroxine has a half-life of 7.5 days when taken daily, so about six weeks is required for it to reach a steady level in the blood.

Propylthiouracil (PTU) is a medication used to treat hyperthyroidism. This includes hyperthyroidism due to Graves' disease and toxic multinodular goiter. In a thyrotoxic crisis it is generally more effective than methimazole. Otherwise it is typically only used when methimazole, surgery, and radioactive iodine is not possible. It is taken by mouth.

Complications of pregnancy are health problems that are related to, or arise during pregnancy. Complications that occur primarily during childbirth are termed obstetric labor complications, and problems that occur primarily after childbirth are termed puerperal disorders. While some complications improve or are fully resolved after pregnancy, some may lead to lasting effects, morbidity, or in the most severe cases, maternal or fetal mortality.
Thyroid disease is a medical condition that affects the function of the thyroid gland. The thyroid gland is located at the front of the neck and produces thyroid hormones that travel through the blood to help regulate many other organs, meaning that it is an endocrine organ. These hormones normally act in the body to regulate energy use, infant development, and childhood development.
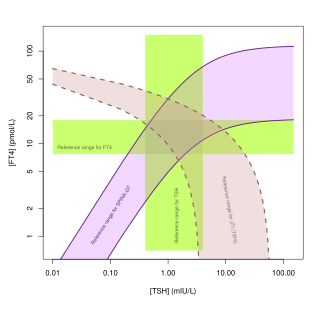
Thyroid function tests (TFTs) is a collective term for blood tests used to check the function of the thyroid. TFTs may be requested if a patient is thought to suffer from hyperthyroidism or hypothyroidism, or to monitor the effectiveness of either thyroid-suppression or hormone replacement therapy. It is also requested routinely in conditions linked to thyroid disease, such as atrial fibrillation and anxiety disorder.
Goitrogens are substances that disrupt the production of thyroid hormones. This triggers the pituitary to release thyroid-stimulating hormone (TSH), which then promotes the growth of thyroid tissue, eventually leading to goiter.
Postpartum thyroiditis refers to thyroid dysfunction occurring in the first 12 months after pregnancy and may involve hyperthyroidism, hypothyroidism or the two sequentially. According to the National Institute of Health, postpartum thyroiditis affects about 8% of pregnancies. There are, however, different rates reported globally. This is likely due to the differing amounts of average postpartum follow times around the world, and due to humans' own innate differences. For example, in Bangkok, Thailand the rate is 1.1%, but in Brazil it is 13.3%. The first phase is typically hyperthyroidism. Then, the thyroid either returns to normal or a woman develops hypothyroidism. Of those women who experience hypothyroidism associated with postpartum thyroiditis, one in five will develop permanent hypothyroidism requiring lifelong treatment.

The hypothalamic–pituitary–thyroid axis is part of the neuroendocrine system responsible for the regulation of metabolism and also responds to stress.
Thyroid hormones are any hormones produced and released by the thyroid gland, namely triiodothyronine (T3) and thyroxine (T4). They are tyrosine-based hormones that are primarily responsible for regulation of metabolism. T3 and T4 are partially composed of iodine, derived from food. A deficiency of iodine leads to decreased production of T3 and T4, enlarges the thyroid tissue and will cause the disease known as simple goitre.
Autoimmune thyroiditis, also known as Hashimoto's disease and chronic lymphocytic thyroiditis, is a chronic disease occurring in the thyroid, the butterfly-shaped endocrine gland in the anterior neck. This disease occurs when the body interprets components of the thyroid glands as threats, therefore producing special antibodies that target the thyroid's cells or proteins, thereby destroying it. It most commonly presents as hypothyroidism with or without a goiter. It is the most common cause of hypothyroidism in iodine-sufficient areas of the world.
Antithyroid autoantibodies (or simply antithyroid antibodies) are autoantibodies targeted against one or more components on the thyroid. The most clinically relevant anti-thyroid autoantibodies are anti-thyroid peroxidase antibodies (anti-TPO antibodies, TPOAb), thyrotropin receptor antibodies (TRAb) and thyroglobulin antibodies (TgAb). TRAb's are subdivided into activating, blocking and neutral antibodies, depending on their effect on the TSH receptor. Anti-sodium/iodide (Anti–Na+/I−) symporter antibodies are a more recent discovery and their clinical relevance is still unknown. Graves' disease and Hashimoto's thyroiditis are commonly associated with the presence of anti-thyroid autoantibodies. Although there is overlap, anti-TPO antibodies are most commonly associated with Hashimoto's thyroiditis and activating TRAb's are most commonly associated with Graves' disease. Thyroid microsomal antibodies were a group of anti-thyroid antibodies; they were renamed after the identification of their target antigen (TPO).
Thyroid's secretory capacity is the maximum stimulated amount of thyroxine that the thyroid can produce in a given time-unit.
References
- 1 2 3 4 Korevaar, Tim I. M.; Medici, Marco; Visser, Theo J.; Peeters, Robin P. (2017-08-04). "Thyroid disease in pregnancy: new insights in diagnosis and clinical management". Nature Reviews. Endocrinology. 13 (10): 610–622. doi:10.1038/nrendo.2017.93. ISSN 1759-5037. PMID 28776582. S2CID 24810888.
- ↑ Okosieme, OE; Marx, H; Lazarus, JH (Sep 2008). "Medical management of thyroid dysfunction in pregnancy and the postpartum". Expert Opinion on Pharmacotherapy. 9 (13): 2281–93. doi:10.1517/14656566.9.13.2281. PMID 18710353. S2CID 71280624.
- ↑ Korevaar, Tim I. M.; de Rijke, Yolanda B.; Chaker, Layal; Medici, Marco; Jaddoe, Vincent W. V.; Steegers, Eric A. P.; Visser, Theo J.; Peeters, Robin P. (March 2017). "Stimulation of Thyroid Function by Human Chorionic Gonadotropin During Pregnancy: A Risk Factor for Thyroid Disease and a Mechanism for Known Risk Factors". Thyroid. 27 (3): 440–450. doi:10.1089/thy.2016.0527. ISSN 1557-9077. PMID 28049387.
- ↑ Spencer, Laura; Bubner, Tanya; Bain, Emily; Middleton, Philippa (2015-09-21). "Screening and subsequent management for thyroid dysfunction pre-pregnancy and during pregnancy for improving maternal and infant health". The Cochrane Database of Systematic Reviews. 2015 (9): CD011263. doi:10.1002/14651858.cd011263.pub2. PMC 9233937 . PMID 26387772.
- 1 2 3 Korevaar, Tim I M; Muetzel, Ryan; Medici, Marco; Chaker, Layal; Jaddoe, Vincent W V; de Rijke, Yolanda B; Steegers, Eric A P; Visser, Theo J; White, Tonya; Tiemeier, Henning; Peeters, Robin P (September 2015). "Association of maternal thyroid function during early pregnancy with offspring IQ and brain morphology in childhood: a population-based prospective cohort study". The Lancet Diabetes & Endocrinology. 4 (1): 35–43. doi:10.1016/s2213-8587(15)00327-7. hdl: 1765/79096 . PMID 26497402.
- ↑ Smyth, PP; Hetherton, AM; Smith, DF; Radcliff, M; O'Herlihy, C (Sep 1997). "Maternal iodine status and thyroid volume during pregnancy: correlation with neonatal iodine intake". The Journal of Clinical Endocrinology and Metabolism. 82 (9): 2840–3. doi: 10.1210/jcem.82.9.4203 . PMID 9284707.
- ↑ WHO S, Andersson M, de Benoist B, Delange F, Zupan J (Dec 2007). "Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: conclusions and recommendations of the Technical Consultation". Public Health Nutrition. 10 (12A): 1606–11. doi: 10.1017/S1368980007361004 . hdl: 20.500.11850/5838 . PMID 18053287.
- ↑ Klein, RZ; Haddow, JE; Faix, JD; Brown, RS; Hermos, RJ; Pulkkinen, A; Mitchell, ML (Jul 1991). "Prevalence of thyroid deficiency in pregnant women". Clinical Endocrinology. 35 (1): 41–6. doi:10.1111/j.1365-2265.1991.tb03494.x. PMID 1889138. S2CID 36178076.
- ↑ Mandel SJ. "Hypothyroidism and chronic autoimmune thyroiditis in the pregnant state: maternal aspects." Best Pract Res Clin Endocrinol Metab. 2004; 18: 213-24.
- ↑ Mandel, SJ (Jun 2004). "Hypothyroidism and chronic autoimmune thyroiditis in the pregnant state: maternal aspects". Best Practice & Research. Clinical Endocrinology & Metabolism. 18 (2): 213–24. doi:10.1016/j.beem.2004.03.006. PMID 15157837.
- ↑ Glinoer, D; Soto, MF; Bourdoux, P; Lejeune, B; Delange, F; Lemone, M; Kinthaert, J; Robijn, C; Grun, JP; de Nayer, P (Aug 1991). "Pregnancy in patients with mild thyroid abnormalities: maternal and neonatal repercussions". The Journal of Clinical Endocrinology and Metabolism. 73 (2): 421–7. doi:10.1210/jcem-73-2-421. PMID 1906897.
- ↑ "Thyroid Disease & Pregnancy". Office on Women's Health, U.S. Department of Health and Human Services. 1 February 2017. Archived from the original on 12 July 2017. Retrieved 9 December 2017.
 This article incorporates text from this source, which is in the public domain .
This article incorporates text from this source, which is in the public domain . - ↑ "Postpartum Thyroiditis" (PDF). American Thyroid Association. 2014. Retrieved 9 December 2017.
- ↑ Davis, LE; Leveno, KJ; Cunningham, FG (Jul 1988). "Hypothyroidism complicating pregnancy". Obstetrics and Gynecology. 72 (1): 108–12. PMID 3380497.
- ↑ Casey, BM; Dashe, JS; Wells, CE; McIntire, DD; Byrd, W; Leveno, KJ; Cunningham, FG (Feb 2005). "Subclinical hypothyroidism and pregnancy outcomes". Obstetrics and Gynecology. 105 (2): 239–45. doi:10.1097/01.AOG.0000152345.99421.22. PMID 15684146. S2CID 11231790.
- ↑ Stagnaro-Green, A; Chen, X; Bogden, JD; Davies, TF; Scholl, TO (Apr 2005). "The thyroid and pregnancy: a novel risk factor for very preterm delivery". Thyroid. 15 (4): 351–7. doi:10.1089/thy.2005.15.351. PMID 15876159.
- ↑ Negro, R; Formoso, G; Mangieri, T; Pezzarossa, A; Dazzi, D; Hassan, H (Jul 2006). "Levothyroxine treatment in euthyroid pregnant women with autoimmune thyroid disease: effects on obstetrical complications". The Journal of Clinical Endocrinology and Metabolism. 91 (7): 2587–91. doi: 10.1210/jc.2005-1603 . PMID 16621910.
- ↑ Haddow, JE; Palomaki, GE; Allan, WC; Williams, JR; Knight, GJ; Gagnon, J; O'Heir, CE; Mitchell, ML; Hermos, RJ; Waisbren, SE; Faix, JD; Klein, RZ (Aug 19, 1999). "Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child". The New England Journal of Medicine. 341 (8): 549–55. doi: 10.1056/NEJM199908193410801 . PMID 10451459. S2CID 4654832.
- ↑ Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ (Sep 2003). "Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study". Clinical Endocrinology. 59 (3): 282–8. doi:10.1046/j.1365-2265.2003.01822.x. PMID 12919150. S2CID 12993173.
- ↑ Pop VJ, de Vries E, van Baar AL, Waelkens JJ, de Rooy HA, Horsten M, Donkers MM, Komproe IH, van Son MM, Vader HL (Dec 1995). "Maternal thyroid peroxidase antibodies during pregnancy: a marker of impaired child development?". The Journal of Clinical Endocrinology and Metabolism. 80 (12): 3561–6. doi:10.1210/jcem.80.12.8530599. PMID 8530599.
- ↑ "Hypothyroidism". National Institute of Diabetes and Digestive and Kidney Diseases. March 2013. Archived from the original on 5 March 2016. Retrieved 9 December 2017.
- ↑ Abalovich M, Amino N, Barbour LA, Cobin RH, De Groot LJ, Glinoer D, Mandel SJ, Stagnaro-Green A (Aug 2007). "Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology and Metabolism. 92 (8 Suppl): S1–47. doi: 10.1210/jc.2007-0141 . PMID 17948378.
- ↑ Velkeniers B, Van Meerhaeghe A, Poppe K, Unuane D, Tournaye H, Haentjens P (May–Jun 2013). "Levothyroxine treatment and pregnancy outcome in women with subclinical hypothyroidism undergoing assisted reproduction technologies: systematic review and meta-analysis of RCTs". Human Reproduction Update. 19 (3): 251–8. doi: 10.1093/humupd/dms052 . PMID 23327883.
- ↑ Marx, H; Amin, P; Lazarus, JH (Mar 22, 2008). "Hyperthyroidism and pregnancy". BMJ (Clinical Research Ed.). 336 (7645): 663–7. doi:10.1136/bmj.39462.709005.AE. PMC 2270981 . PMID 18356235.
- ↑ Swaminathan, R. (2000-07-01). "Thyroid Function during Pregnancy". Clinical Chemistry. 46 (7): 1016–1017. doi: 10.1093/clinchem/46.7.1016 . ISSN 0009-9147. PMID 10894853.
- ↑ Zimmerman D (1999). "Fetal and neonatal hyperthyroidism". Thyroid. 9 (7): 727–33. doi:10.1089/thy.1999.9.727. PMID 10447021.
- ↑ Polak M, Le Gac I, Vuillard E, et al. (2004). "Fetal and neonatal thyroid function in relation to maternal Graves' disease". Best Pract Res Clin Endocrinol Metab. 18 (2): 289–302. doi:10.1016/s1521-690x(04)00019-3. PMID 15157841.
- ↑ Mestman JH (2004). "Hyperthyroidism in pregnancy". Best Practice & Research: Clinical Endocrinology & Metabolism. 18 (2): 267–88. doi:10.1016/j.beem.2004.03.005. PMID 15157840.
- ↑ Fumarola, A; Di Fiore, A; Dainelli, M; Grani, G; Carbotta, G; Calvanese, A (June 2011). "Therapy of hyperthyroidism in pregnancy and breastfeeding". Obstetrical & Gynecological Survey. 66 (6): 378–85. doi:10.1097/ogx.0b013e31822c6388. PMID 21851752. S2CID 28728514.
- ↑ Vissenberg, R.; Van Den Boogaard, E.; Van Wely, M.; Van Der Post, J. A.; Fliers, E.; Bisschop, P. H.; Goddijn, M. (2012). "Treatment of thyroid disorders before conception and in early pregnancy: A systematic review". Human Reproduction Update. 18 (4): 360–73. doi: 10.1093/humupd/dms007 . PMID 22431565.
- ↑ Mandel, SJ; Cooper, DS (Jun 2001). "The use of antithyroid drugs in pregnancy and lactation". The Journal of Clinical Endocrinology and Metabolism. 86 (6): 2354–9. doi: 10.1210/jcem.86.6.7573 . PMID 11397822.
- ↑ Muller, AF; Drexhage, HA; Berghout, A (Oct 2001). "Postpartum thyroiditis and autoimmune thyroiditis in women of childbearing age: recent insights and consequences for antenatal and postnatal care". Endocrine Reviews. 22 (5): 605–30. doi: 10.1210/edrv.22.5.0441 . PMID 11588143.
- ↑ "Hypothyroidism". The Lecturio Medical Concept Library. Retrieved 27 July 2021.
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||