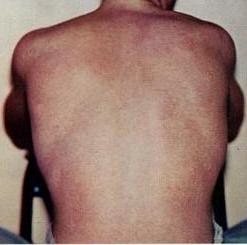
Dengue fever is a mosquito-borne tropical disease caused by the dengue virus. Symptoms typically begin three to fourteen days after infection. These may include a high fever, headache, vomiting, muscle and joint pains, and a characteristic skin itching and skin rash. Recovery generally takes two to seven days. In a small proportion of cases, the disease develops into a more severe dengue hemorrhagic fever, resulting in bleeding, low levels of blood platelets and blood plasma leakage, or into dengue shock syndrome, where dangerously low blood pressure occurs.

After the Bolivarian Revolution, extensive inoculation programs and the availability of low- or no-cost health care provided by the Venezuelan Institute of Social Security made Venezuela's health care infrastructure one of the more advanced in Latin America.

Chikungunya is a mosquito-borne alpha virus that was first isolated after a 1952 outbreak in modern-day Tanzania. The virus has circulated in forested regions of sub-Saharan African in cycles involving nonhuman primate hosts and arboreal mosquito vectors. Phylogenetic studies indicate that the urban transmission cycle—the transmission of a pathogen between humans and mosquitoes that exist in urban environments—was established on multiple occasions from strains occurring on the eastern half of Africa in non-human primate hosts. This emergence and spread beyond Africa may have started as early as the 18th century. Currently, available data does not indicate whether the introduction of chikungunya into Asia occurred in the 19th century or more recently, but this epidemic Asian strain causes outbreaks in India and continues to circulate in Southeast Asia.
Globalization, the flow of information, goods, capital, and people across political and geographic boundaries, allows infectious diseases to rapidly spread around the world, while also allowing the alleviation of factors such as hunger and poverty, which are key determinants of global health. The spread of diseases across wide geographic scales has increased through history. Early diseases that spread from Asia to Europe were bubonic plague, influenza of various types, and similar infectious diseases.
A reverse zoonosis, also known as a zooanthroponosis or anthroponosis, is a pathogen reservoired in humans that is capable of being transmitted to non-human animals.
Aircraft disinsection is the use of insecticide on international flights and in other closed spaces for insect and disease control. Confusion with disinfection, the elimination of microbes on surfaces, is not uncommon. Insect vectors of disease, mostly mosquitoes, have been introduced into and become indigenous in geographic areas where they were not previously present. Dengue, chikungunya and Zika spread across the Pacific and into the Americas by means of the airline networks. Cases of "airport malaria", in which live malaria-carrying mosquitoes disembark and infect people near the airport, may increase with global warming.

Pakistan is the fifth most populous country in the world with population approaching 225 million. It is a developing country struggling in many domains due to which the health system has suffered a lot. As a result of that, Pakistan is ranked 122nd out of 190 countries in the World Health Organization performance report.

Thailand has had "a long and successful history of health development," according to the World Health Organization. Life expectancy is averaged at seventy years. Non-communicable diseases form the major burden of morbidity and mortality, while infectious diseases including malaria and tuberculosis, as well as traffic accidents, are also important public health issues.
HIV/AIDS in Bolivia has a less than 1 percent prevalence of Bolivia's adult population estimated to be HIV-positive. Bolivia has one of the lowest HIV prevalence rates in the Latin America and Caribbean region.

Mosquito-borne diseases or mosquito-borne illnesses are diseases caused by bacteria, viruses or parasites transmitted by mosquitoes. Nearly 700 million people get a mosquito-borne illness each year resulting in over 725,000 deaths.

The quality of health in Cambodia is rising along with its growing economy. The public health care system has a high priority from the Cambodian government and with international help and assistance, Cambodia has seen some major and continuous improvements in the health profile of its population since the 1980s, with a steadily rising life expectancy.

Bangladesh is one of the most populous countries in the world, as well as having one of the fastest growing economies in the world. Consequently, Bangladesh faces challenges and opportunities in regards to public health. A remarkable metamorphosis has unfolded in Bangladesh, encompassing the demographic, health, and nutritional dimensions of its populace.

As of 2010, dengue fever is believed to infect 50 to 100 million people worldwide a year with 1/2 million life-threatening infections. It dramatically increased in frequency between 1960 and 2010, by 30 fold. This increase is believed to be due to a combination of urbanization, population growth, increased international travel, and global warming. The geographical distribution is around the equator with 70% of the total 2.5 billion people living in endemic areas from Asia and the Pacific. Many of the infected people during outbreaks are not virally tested, therefore their infections may also be due to chikungunya, a coinfection of both, or even other similar viruses.
Even though Panama has one of the fastest growing economies in the western hemisphere, an estimated 500,000 people are in extreme poverty. Panama has major socioeconomic and health inequalities between the country’s urban and rural populations. The indigenous population lives in more disadvantaged conditions and experiences greater vulnerability in health. In general, the population living in more marginalized areas has less service coverage and less access to health care.
The United States Intelligence Community (IC) has a long history of producing assessments on infectious diseases. Most of these papers are distributed to government administrators and inform the choices of policymakers. Three of these assessments stand out as analytical products that have had important impact on the awareness, funding and treatment of infectious diseases around the world. The first paper is the National Intelligence Estimate on the Global Infectious Disease Threat, the second paper is the assessment on the Next Wave of HIV/AIDS, and the third paper was the assessment on SARS. This page summarizes the findings of these three papers and provides information about their impact.
The 2013–2014 chikungunya outbreak represented the first recorded outbreak of the disease outside of tropical Africa and Asia. In December 2013, the first locally transmitted case of chikungunya in the Americas was detected in Saint Martin. Shortly after the first case the disease began to spread rapidly throughout the Caribbean region. By the end of the year, it had spread to Martinique and Guadeloupe, with suspected cases in Saint Barthélemy. By the end of January 2014, cases had been confirmed in Saint Barthélemy, as well as the British Virgin Islands, Dominica, and French Guiana. On the basis of 4,000 confirmed cases and over 30,000 suspected cases, the Caribbean Public Health Agency (CARPHA) declared a Caribbean-wide epidemic of the virus in early May. By the end of May, four cases of chikungunya had been confirmed in Florida. By July 2014 there were an estimated 355,000 cases in the Caribbean. By August 2014, 25 Caribbean countries had confirmed at least one case. The epidemic was over by 2015.

Ebola virus disease in Mali occurred in October 2014, leading to concern about the possibility of an outbreak of Ebola in Mali. A child was brought from Guinea and died in the northwestern city of Kayes. Mali contact traced over 100 people who had contact with the child; tracing was completed in mid-November with no further cases discovered. In November, a second unrelated outbreak occurred in Mali's capital city, Bamako. Several people at a clinic are thought to have been infected by a man traveling from Guinea. On January 18, Mali was declared Ebola-free after 42 days with no new cases. There had been a cumulative total of eight cases with six deaths.
The Norwegian Institute of Public Health is responsible for maintaining and revising the list of notifiable diseases in Norway and participates in the European Centre for Disease Prevention and Control (ECDC) and the World Health Organization's surveillance of infectious diseases. The notifiable diseases are classified into Group A, Group B and Group C diseases, depending on the procedure for reporting the disease.
A notifiable disease is one which the law requires to be reported to government authorities.

