
In vertebrates, the gallbladder, also known as the cholecyst, is a small hollow organ where bile is stored and concentrated before it is released into the small intestine. In humans, the pear-shaped gallbladder lies beneath the liver, although the structure and position of the gallbladder can vary significantly among animal species. It receives bile, produced by the liver, via the common hepatic duct, and stores it. The bile is then released via the common bile duct into the duodenum, where the bile helps in the digestion of fats.

A bile duct is any of a number of long tube-like structures that carry bile, and is present in most vertebrates. The bile duct is separated into three main parts: the fundus (superior), the body (middle), and the neck (inferior).

Cholecystectomy is the surgical removal of the gallbladder. Cholecystectomy is a common treatment of symptomatic gallstones and other gallbladder conditions. In 2011, cholecystectomy was the eighth most common operating room procedure performed in hospitals in the United States. Cholecystectomy can be performed either laparoscopically, or via an open surgical technique.

Biliary atresia, also known as extrahepatic ductopenia and progressive obliterative cholangiopathy, is a childhood disease of the liver in which one or more bile ducts are abnormally narrow, blocked, or absent. It can be congenital or acquired. It has an incidence of one in 10,000–15,000 live births in the United States, and a prevalence of one in 16,700 in the British Isles. Biliary atresia is most common in East Asia, with a frequency of one in 5,000.

Cholangiocarcinoma, also known as bile duct cancer, is a type of cancer that forms in the bile ducts. Symptoms of cholangiocarcinoma may include abdominal pain, yellowish skin, weight loss, generalized itching, and fever. Light colored stool or dark urine may also occur. Other biliary tract cancers include gallbladder cancer and cancer of the ampulla of Vater.

A pancreaticoduodenectomy, also known as a Whipple procedure, is a major surgical operation most often performed to remove cancerous tumours from the head of the pancreas. It is also used for the treatment of pancreatic or duodenal trauma, or chronic pancreatitis. Due to the shared blood supply of organs in the proximal gastrointestinal system, surgical removal of the head of the pancreas also necessitates removal of the duodenum, proximal jejunum, gallbladder, and, occasionally, part of the stomach.

Alagille syndrome (ALGS) is a genetic disorder that affects primarily the liver and the heart. Problems associated with the disorder generally become evident in infancy or early childhood. The disorder is inherited in an autosomal dominant pattern, and the estimated prevalence of Alagille syndrome is 1 in every 30,000 to 1 in every 40,000 live births. It is named after the French pediatrician Daniel Alagille, who first described the condition in 1969. Children with Alagille syndrome live to the age of 18 in about 90% of the cases.

Pediatric surgery is a subspecialty of surgery involving the surgery of fetuses, infants, children, adolescents, and young adults.
The Kocher manoeuvre is a surgical procedure to expose structures in the retroperitoneum behind the duodenum and pancreas. In vascular surgery, it is described as a method to expose the abdominal aorta. It usually has been in contrast to midline laparotomy and right retroperitoneal space dissection. These two procedures have been used for diverse cases, but have approximately equivalent outcomes.
Cholangiocytes are the epithelial cells of the bile duct. They are cuboidal epithelium in the small interlobular bile ducts, but become columnar and carbonate-secreting in larger bile ducts approaching the porta hepatis and the extrahepatic ducts. They contribute to hepatocyte survival by transporting bile acids.
An accessory bile duct is a conduit that transports bile and is considered to be supernumerary or auxiliary to the biliary tree.
Neonatal cholestasis refers to elevated levels of conjugated bilirubin identified in newborn infants within the first few months of life. Conjugated hyperbilirubinemia is clinically defined as >20% of total serum bilirubin or conjugated bilirubin concentration greater than 1.0 mg/dL regardless of total serum bilirubin concentration. The differential diagnosis for neonatal cholestasis can vary extensively. However, the underlying disease pathology is caused by improper transport and/or defects in excretion of bile from hepatocytes leading to an accumulation of conjugated bilirubin in the body. Generally, symptoms associated with neonatal cholestasis can vary based on the underlying cause of the disease. However, most infants affected will present with jaundice, scleral icterus, failure to thrive, acholic or pale stools, and dark urine.

Percutaneous transhepatic cholangiography, percutaneous hepatic cholangiogram (PTHC) is a radiological technique used to visualize the anatomy of the biliary tract. A contrast medium is injected into a bile duct in the liver, after which X-rays are taken. It allows access to the biliary tree in cases where endoscopic retrograde cholangiopancreatography has been unsuccessful. Initially reported in 1937, the procedure became popular in 1952.
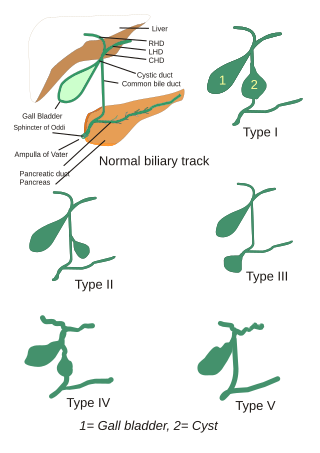
Choledochal cysts are congenital conditions involving cystic dilatation of bile ducts. They are uncommon in western countries but not as rare in East Asian nations like Japan and China.

The liver is a major metabolic organ only found in vertebrate animals, which performs many essential biological functions such as detoxification of the organism, and the synthesis of proteins and biochemicals necessary for digestion and growth. In humans, it is located in the right upper quadrant of the abdomen, below the diaphragm and mostly shielded by the lower right rib cage. Its other metabolic roles include carbohydrate metabolism, the production of hormones, conversion and storage of nutrients such as glucose and glycogen, and the decomposition of red blood cells.
Cholecystostomy or (cholecystotomy) is a medical procedure used to drain the gallbladder through either a percutaneous or endoscopic approach. The procedure involves creating a stoma in the gallbladder, which can facilitate placement of a tube or stent for drainage, first performed by American surgeon, Dr. John Stough Bobbs, in 1867. It is sometimes used in cases of cholecystitis or other gallbladder disease where the person is ill, and there is a need to delay or defer cholecystectomy. The first endoscopic cholecystostomy was performed by Drs. Todd Baron and Mark Topazian in 2007 using ultrasound guidance to puncture the stomach wall and place a plastic biliary catheter for gallbladder drainage.

A biloma is a circumscribed abdominal collection of bile outside the biliary tree. It occurs when there is excess bile in the abdominal cavity. It can occur during or after a bile leak. There is an increased chance of a person developing biloma after having a gallbladder removal surgery, known as laparoscopic cholecystectomy. This procedure can be complicated by biloma with incidence of 0.3–2%. Other causes are liver biopsy, abdominal trauma, and, rarely, spontaneous perforation. The formation of biloma does not occur frequently. Biliary fistulas are also caused by injury to the bile duct and can result in the formation of bile leaks. Biliary fistulas are abnormal communications between organs and the biliary tract. Once diagnosed, they usually require drainage. The term "biloma" was first coined in 1979 by Gould and Patel. They discovered it in a case with extrahepatic bile leakage. The cause of this was trauma to the upper right quadrant of the abdomen. Originally, biloma was described as an "encapsulated collection" of extrahepatic bile. Biloma is now described as extrabiliary collections of bile that can be either intrahepatic or extrahepatic. The most common cause of biloma is trauma to the liver. There are other causes such as abdominal surgery, endoscopic surgery and percutaneous catheter drainage. Injury and abdominal trauma can cause damage to the biliary tree. The biliary tree is a system of vessels that direct secreations from the liver, gallbladder, and pancreas through a series of ducts into the duodenum. This can result in a bile leak which is a common cause of the formation of biloma. It is possible for biloma to be associated with mortality, though it is not common. Bile leaks occur in about one percent of causes.

Morio Kasai was a Japanese surgeon who had a strong interest in pediatric surgery. While Kasai went into practice at a time when pediatric surgery was not an established subspecialty, much of his clinical and research work was related to the surgical care of children. He is best known for devising a surgical procedure, the hepatoportoenterostomy, to address a life-threatening birth defect known as biliary atresia. The modern form of the operation is still known as the Kasai procedure.

Choledochoduodenostomy (CDD) is a surgical procedure to create an anastomosis, a surgical connection, between the common bile duct (CBD) and an alternative portion of the duodenum. In healthy individuals, the CBD meets the pancreatic duct at the ampulla of Vater, which drains via the major duodenal papilla to the second part of duodenum. In cases of benign conditions such as narrowing of the distal CBD or recurrent CBD stones, performing a CDD provides the diseased patient with CBD drainage and decompression. A side-to-side anastomosis is usually performed.
Deirdre Kelly is an Irish clinician, academic, and author. She is Professor of Paediatric Hepatology at the University of Birmingham and Clinical Lead for National Paediatric Hepatitis C Operational Delivery Network. She chairs the Board of Pension Trustees at the General Medical Council and is a non-executive director at NHS Blood and Transplant.
