Procedure

After pyloric stenosis is identified in a patient, and any electrolyte and fluid imbalances are stabilized, the surgeon will perform the procedure. [4] [1] During which, the surgeon must access the pylorus through the abdominal wall. This can either be done laparoscopically or with an "open" procedure. In either case, the once the pylorus is accessed, the surgeon will visualize the hypertrophied pyloric muscle. Then, the surgeon will carefully cut through the outer layers of tissue and through the pyloric muscle to the mucosa, which is the layer of tissue facing the inside of the gastrointestinal tract. From there, the two portions of the pyloric muscle are tested for mobility and the mucosal layer is inspected for any unintentional damage. Depending on the approach, the pylorus, stomach, and gastrointestinal tract are returned to their appropriate place in the abdominal cavity and the medical equipment is removed. Finally, each of the surgical incisions are stitched closed and the patient is taken back to post-operative area for monitoring. [5] [4]
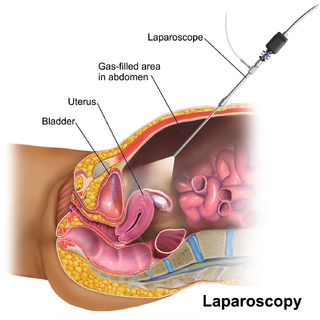
Laparoscopic approach: In the laparoscopic approach, the appropriate area of the gastrointestinal tract is accessed in a minimally invasive manner. [5] This approach may be chosen due to the reduced hospital stay, quicker recovery time, and higher satisfaction with the appearance of the surgical site after the patient has healed when compared to the older open approach. [2] Typically, two to three trocars, a medical device used to penetrate the abdominal wall in laparoscopic medical procedures, are placed in their appropriate positions. This is typically done by making a small cut for each trocar in the abdominal wall before placing the trocar into the cut. The abdomen is then filled with a gas, such as carbon dioxide to increase visibility with the laparoscopic camera and increase working space. [1] Once the laparoscopic instruments and camera are place through the trocars, the hypertrophied pylorus is visualized. Then, the pyloric muscle is cut down to the mucosa and the muscle fibers are spread apart using the laparoscopic instruments. From there, the two pyloric sections are tested independently for appropriate movement. After that, the mucosa is inspected for any unintentional damaged. This is done by inflating the patient's stomach and looking for the formation of bubbles along the mucosa. [4] If a leak is identified it is typically repaired with sutures if determined to be appropriate. Finally, all instruments and trocars are removed before the surgical wound sites are repaired with stitches. [5]

Open approach: In the older open pyloromyotomy, the appropriate area of the gastrointestinal tract is accessed by creating a single cut on the abdomen of the patient and the pylorus and stomach are gently pulled through the opening for the procedure. [5] This approach may be chosen due to patient/parent preference or if determined by the surgeon to be more appropriate. [6] Once the initial cut on the abdomen is made, a layer of connective tissue between the abdomen and stomach is cut through. Then, the stomach and pylorus are carefully pulled through the opening created by the initial cut and the hypertrophied pylorus is identified by the surgeon. After that, the pyloric muscle is cut down to the mucosa and the muscle fibers are spread apart using a pyloric spreader. The newly separated pyloric sections are tested for adequate movement and the mucosa is tested for holes or other damage, which are repaired using suture as appropriate. Finally, the stomach and pylorus are carefully placed back into the abdominal cavity and the various tissue layers are repaired with stitches. [5]