Mean arterial pressure (MAP) is an average calculated blood pressure in an individual during a single cardiac cycle.[1] Although methods of estimating MAP vary, a common calculation is to take one-third of the pulse pressure (the difference between the systolic and diastolic pressures), and add that amount to the diastolic pressure.[2][3] A normal MAP is about 90 mmHg.[4]
The mean arterial pressure is calculated as the sum of the diastolic blood pressure plus the difference of the systolic pressure to the diastolic pressure, with the difference divided by three, as shown in the equation below.
For example, a diastolic pressure of 70 mm Hg and a systolic pressure of 100 mm Hg would yield by means of the calculator below a MAP of 80 mm Hg.
Mean arterial pressure can be measured directly or estimated from systolic and diastolic blood pressure by using a formula.[5]
In the direct approach, mean arterial pressure can be calculated exactly using an arterial catheter with a transducer; this device inserted into the bloodstream measures arterial pressure over time.
A less exact but less invasive approach is to use a blood pressure cuff or an oscillometric blood pressure device to determine systolic and diastolic blood pressure; these values can be plugged into a formula to estimate mean arterial pressure.[6]
Estimating
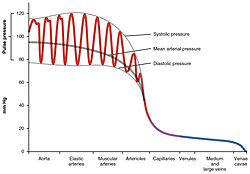
Mean arterial pressure in relation to systolic and diastolic pressure in blood vessels
While MAP can only be measured directly by invasive monitoring, there are several formulas for estimating MAP in terms of easy-to-measure quantities such as systolic and diastolic blood pressure.
One common formula is to double the lower (diastolic) blood pressure, add it to the higher (systolic) blood pressure, and divide the resulting sum by 3 to estimate MAP:[2]
This is equivalent to taking one-third of the pulse pressure (systolic minus diastolic pressure) and adding it to the diastolic pressure:[2][3][7]
where:
DP = diastolic pressure
SP = systolic pressure
MAP = mean arterial pressure
Systolic pressure minus diastolic pressure equals the pulse pressure which may be substituted in.[5]
Blood pressure cuff
Another way to find the MAP is to use the systemic vascular resistance equated (), which is represented mathematically by the formula
where is the change in pressure across the systemic circulation from its beginning to its end and is the flow through the vasculature (equal to cardiac output).
In other words:
Therefore, MAP can be determined by rearranging the equation to:
At high heart rates is more closely approximated by the arithmetic mean of systolic and diastolic pressures because of the change in shape of the arterial pressure pulse.
For a more accurate formula of for elevated heart rates use:
PP = pulse pressure which is systolic minus diastolic pressure[11]
Most accurate
The version of the MAP equation multiplying 0.412 by pulse pressure and adding diastolic blood is indicated to correlate better than other versions of the equation with left ventricular hypertrophy, carotid wall thickness and aortic stiffness.[12] It is expressed:
where:
DBP = diastolic pressure
MAP = mean arterial pressure
PP = pulse pressure
Young patients
For young patients with congenital heart disease a slight alteration to the factor used found to be more precise. This was written as:
where:
DBP = diastolic pressure
MAP = mean arterial pressure
PP = pulse pressure
This added precision means cerebral blood flow can be more accurately maintained in uncontrolled hypertension.[13]
Neonates
For neonates, because of their altered physiology, a different formula has been proposed for a more precise reading:
where:
DBP = diastolic pressure
MAP = mean arterial pressure
PP = pulse pressure
It has also been suggested that when getting readings from a neonates radial arterial line, mean arterial pressure can be approximated by averaging the systolic and diastolic pressure.[14]
Other formula versions
Other formulas used to estimate mean arterial pressure are:
When assessing hypotension, the context of the baseline blood pressure needs to be considered. Acute decreases in mean arterial pressure of around 25% put people at increased risk for organ damage and potential mortality.[19] Even one minute at a MAP of 50 mmHg, or accumulative effects over short periods, increases the risk of mortality by 5%, and can result in organ failure or complications.[20][21]
In people hospitalized with shock, a MAP of 65 mmHg lasting for more than two hours was associated with higher mortality.[22] In people with sepsis, the vasopressor dosage may be titrated on the basis of estimated MAP.[2]
MAP may be used like systolic blood pressure in monitoring and treating target blood pressure. Both are used as targets for assessing sepsis, major trauma, stroke, and intracranial bleeding.[23]
Hypertension
In younger people, elevated MAP is used more commonly than pulse pressure in the prediction of stroke. However in older people, MAP is less predictive of stroke and a better predictor of cardiovascular disease.[24][25]
↑ Razminia M, Trivedi A, Molnar J, Elbzour M, Guerrero M, Salem Y, etal. (December 2004). "Validation of a new formula for mean arterial pressure calculation: the new formula is superior to the standard formula". Catheterization and Cardiovascular Interventions. 63 (4): 419–425. doi:10.1002/ccd.20217. PMID15558774. S2CID25022922.
↑ Chemla D, Hébert JL, Aptecar E, Mazoit JX, Zamani K, Frank R, etal. (July 2002). "Empirical estimates of mean aortic pressure: advantages, drawbacks and implications for pressure redundancy". Clinical Science. 103 (1): 7–13. doi:10.1042/cs1030007. PMID12095398.
↑ Jones D, Francesco L (2017). "Hypotension". In McKean SC, Ross JJ, Dressler DD, Scheurer DB (eds.). Principles and Practice of Hospital Medicine (2nded.). McGraw Hill. ISBN978-0-07-184313-3.
↑ Nicklas JY, Beckmann D, Killat J, Petzoldt M, Reuter DA, Rösch T, Saugel B (February 2019). "Continuous noninvasive arterial blood pressure monitoring using the vascular unloading technology during complex gastrointestinal endoscopy: a prospective observational study". Journal of Clinical Monitoring and Computing. 33 (1): 25–30. doi:10.1007/s10877-018-0131-6. PMID29556885. S2CID4025532.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.