Bronchopulmonary dysplasia (BPD; part of the spectrum of chronic lung disease of infancy) is a chronic lung disease which affects premature infants. Premature (preterm) infants who require treatment with supplemental oxygen or require long-term oxygen are at a higher risk.[1] The alveoli that are present tend to not be mature enough to function normally.[2] It is also more common in infants with low birth weight (LBW) and those who receive prolonged mechanical ventilation to treat respiratory distress syndrome. It results in significant morbidity and mortality. The definition of bronchopulmonary dysplasia has continued to evolve primarily due to changes in the population, such as more survivors at earlier gestational ages, and improved neonatal management including surfactant, antenatal glucocorticoid therapy, and less aggressive mechanical ventilation.[3]
Currently the description of bronchopulmonary dysplasia includes the grading of its severity into mild, moderate and severe. This correlates with the infant's maturity, growth and overall severity of illness.[4] The new system offers a better description of underlying pulmonary disease and its severity.[5]
Discovery
In 1967, William Northway, Robert Rosan, and David Porter first coined the term bronchopulmonary dysplasia "to describe a chronic form of injury to the lungs caused by barotrauma and oxygen injury in preterm infants requiring mechanical ventilation."[6] The disease was first observed three years earlier among premature infants treated with high-concentration oxygen and intermittent positive pressure ventilation, noted by neonatologist Philip Sunshine at Stanford University Medical Center.[7]
Presentation
Complications
Feeding problems are common in infants with bronchopulmonary dysplasia, often due to prolonged intubation. Such infants often display oral-tactile hypersensitivity (also known as oral aversion).[8]
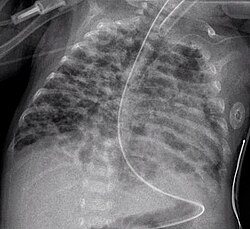
CXR shows with hyperinflation, low diaphragm, atelectasis, cystic changes.
Cause
Prolonged high oxygen delivery in premature infants causes necrotizing bronchiolitis and alveolar septal injury, with inflammation and scarring. This results in hypoxemia. Today, with the advent of surfactant therapy and high frequency ventilation and oxygen supplementation, infants with BPD experience much milder injury without necrotizing bronchiolitis or alveolar septal fibrosis. Instead, there are usually uniformly dilated acini with thin alveolar septa and little or no interstitial fibrosis. It develops most commonly in the first four weeks after birth.[9] Bronchopulmonary dysplasia is now known to be due to abnormal wound healing in response to injury;[10] it has been linked to alterations in the Wnt/beta-catenin pathway.[11][12]
Diagnosis
Earlier criteria
The classic diagnosis of bronchopulmonary dysplasia may be assigned at 28 days of life if the following criteria are met:[citation needed]
Positive pressure ventilation during the first two weeks of life for a minimum of three days.
Clinical signs of abnormal respiratory function.
Requirements for supplemental oxygen for longer than 28 days of age to maintain PaO2 above 50mm Hg.
Chest radiograph with diffuse abnormal findings characteristic of bronchopulmonary dysplasia.
Newer criteria
The 2006 National Institute of Health (US) criteria for BPD (for neonates treated with more than 21% oxygen for at least 28 days)[13] is as follows:[14][15]
Mild
Breathing room air at 36 weeks' post-menstrual age or discharge (whichever comes first) for babies born before 32 weeks, or
breathing room air by 56 days' postnatal age, or discharge (whichever comes first) for babies born after 32 weeks' gestation.
Moderate
Need for <30% oxygen at 36 weeks' postmenstrual age, or discharge (whichever comes first) for babies born before 32 weeks, or
need for <30% oxygen to 56 days' postnatal age, or discharge (whichever comes first) for babies born after 32 weeks' gestation.
Severe
Need for >30% oxygen, with or without positive pressure ventilation or continuous positive pressure at 36 weeks' postmenstrual age, or discharge (whichever comes first) for babies born before 32 weeks, or
need for >30% oxygen with or without positive pressure ventilation or continuous positive pressure at 56 days' postnatal age, or discharge (whichever comes first) for babies born after 32 weeks' gestation.
Management
Infants with bronchopulmonary dysplasia are often treated with diuretics that decrease fluid in the alveoli where gas exchange occurs and bronchodilators that relax the airway muscles to facilitate breathing.[16] To alleviate bronchopulmonary dysplasia, caffeine is another commonly used treatment that reduces inflammation and increases lung volume thereby improving extubation success and decreasing the duration of mechanical ventilation.[17] Viral immunization is important for these children who have a higher risk of infections in the respiratory tract.[18]
Corticosteroid treatment
There is evidence that steroids (systemic corticosteroid treatment) given to babies less than seven days old can prevent bronchopulmonary dysplasia.[19] This treatment increases the risk of neurodevelopmental sequelae (cerebral palsy) and gastrointestinal perforation.[19]
For babies seven days old and older, "late systemic postnatal corticosteroid treatment" may reduce the risk of death and of bronchopulmonary dysplasia.[20] There is some evidence that this treatment does not increase the risk of cerebral palsy, however, long-term studies considering the neurodevelopmental outcomes is needed to further understand the risk of this treatment option.[20] Late systemic postnatal corticosteroid treatment is therefore only recommended for babies seven days old or older who cannot be taken off of a ventilator.[20] The benefit and risks of systemic corticosteroid treatment in older babies who are not intubated (on a ventilator) is not known.[20]
Vitamin A
Vitamin A treatment in low birth weight babies may improve the 36-week mortality risk, decrease the days of mechanical ventilation, and decrease the incidence of bronchopulmonary dysplasia.[21]
Other
Oxygen therapy at home is recommended in those with significant low oxygen levels.[22]
Hypercarbia (too much carbon dioxide in the blood) may contribute to the development of bronchopulmonary dysplasia.[23] Monitoring the level of carbon dioxide in neonatal infants to ensure that the level is not too high or too low (hypocarbia) is important for improving outcomes for neonates in intensive care.[24] Carbon dioxide can be monitored by taking a blood sample (arterial blood gas), through the breath (exhalation), and it can be measured continuously through the skin by using a minimally invasive transcutaneous device.[24] The most effective and safest approach for measuring carbon dioxide in newborn infants is not clear.[24]
It is not clear if treatment with superoxide dimutase supplementation is effective at preventing bronchopulmonary dysplasia in infants born preterm or at reducing preterm infant mortality.[25]
Epidemiology
The rate of BPD varies among institutions, which may reflect neonatal risk factors, care practices (e.g., target levels for acceptable oxygen saturation), and differences in the clinical definitions of BPD.[26][27][28]
↑ Northway Jr, WH; Rosan, RC; Porter, DY (Feb 16, 1967). "Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia". The New England Journal of Medicine. 276 (7): 357–68. doi:10.1056/NEJM196702162760701. PMID5334613.
↑ Sahni, R; Ammari, A; Suri, MS; Milisavljevic, V; Ohira-Kist, K; Wung, JT; Polin, RA (Jan 2005). "Is the new definition of bronchopulmonary dysplasia more useful?". Journal of Perinatology. 25 (1): 41–6. doi:10.1038/sj.jp.7211210. PMID15538399. S2CID22550494.
↑ Ehrenkranz, RA; Walsh, MC; Vohr, BR; Jobe, AH; Wright, LL; Fanaroff, AA; Wrage, LA; Poole, K; National Institutes of Child Health and Human Development Neonatal Research, Network (Dec 2005). "Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia". Pediatrics. 116 (6): 1353–60. doi:10.1542/peds.2005-0249. PMID16322158. S2CID21228956.
↑ National Heart, Lung, and Blood Institute (1998). Bronchopulmonary Dysplasia. National Institutes of Health. p.2.{{cite book}}: CS1 maint: multiple names: authors list (link)
↑ Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR, etal. (2007). "Trends in neonatal morbidity and mortality for very low birthweight infants". Am J Obstet Gynecol. 196 (2): 147.e1–8. doi:10.1016/j.ajog.2006.09.014. PMID17306659. S2CID27489509.
↑ Van Marter LJ, Allred EN, Pagano M, Sanocka U, Parad R, Moore M, etal. (2000). "Do clinical markers of barotrauma and oxygen toxicity explain interhospital variation in rates of chronic lung disease? The Neonatology Committee for the Developmental Network". Pediatrics. 105 (6): 1194–201. doi:10.1542/peds.105.6.1194. PMID10835057.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.