| Neonatal jaundice | |
|---|---|
| Other names | Neonatal hyperbilirubinemia, neonatal icterus, jaundice in newborns |
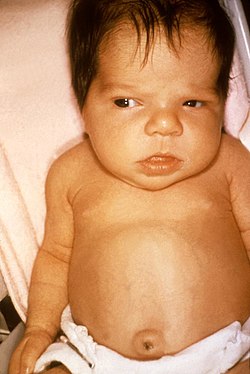 | |
| Jaundice in a newborn | |
| Specialty | Pediatrics |
| Symptoms | Yellowish discoloration of the skin and white part of the eyes [1] |
| Complications | Seizures, cerebral palsy, kernicterus [1] |
| Usual onset | Newborns [1] |
| Types | Physiologic, pathologic [1] |
| Causes | Red blood cell breakdown, liver disease, infection, hypothyroidism, metabolic disorders [2] [1] |
| Diagnostic method | Based on symptoms, confirmed by bilirubin [1] |
| Treatment | More frequent feeding, phototherapy, exchange transfusions [1] |
| Frequency | >50% of babies [1] |
Neonatal jaundice is a yellowish discoloration of the white part of the eyes and skin in a newborn baby due to high bilirubin levels. [1] Other symptoms may include excess sleepiness or poor feeding. [1] Complications may include seizures, cerebral palsy, or bilirubin encephalopathy. [1]
Contents
- Sign and symptoms
- Complications
- Causes
- Unconjugated
- Conjugated (Direct)
- Non-organic causes
- Physiological jaundice
- Diagnosis
- Transcutaneous bilirubinometer
- Pathological jaundice
- Treatment
- Phototherapy
- Exchange transfusions
- Research
- References
- External links
In most cases, there is no specific underlying physiologic disorder. [2] In other cases it results from red blood cell breakdown, liver disease, infection, hypothyroidism, or metabolic disorders (pathologic). [2] [1] A bilirubin level more than 34 μmol/L (2 mg/dL) may be visible. [1] Concerns, in otherwise healthy babies, occur when levels are greater than 308 μmol/L (18 mg/dL), jaundice is noticed in the first day of life, there is a rapid rise in levels, jaundice lasts more than two weeks, or the baby appears unwell. [1] In those with concerning findings further investigations to determine the underlying cause are recommended. [1]
The need for treatment depends on bilirubin levels, the age of the child, and the underlying cause. [1] [3] Treatments may include more frequent feeding, phototherapy, or exchange transfusions. [1] In those who are born early more aggressive treatment tends to be required. [1] Physiologic jaundice generally lasts less than seven days. [1] The condition affects over half of babies in the first week of life. [1] Of babies that are born early about 80% are affected. [2] Globally over 100,000 late-preterm and term babies die each year as a result of jaundice. [4]
