Related Research Articles

Obesity is a condition in which excess body fat has accumulated to such an extent that it may have a negative effect on health. People are classified as obese when their body mass index (BMI)—a measurement obtained by dividing a person's weight by the square of the person's height —is over 30 kg/m2; the range 25–30 kg/m2 is defined as overweight. Some East Asian countries use lower values to calculate obesity.
Lifestyle diseases can be defined as diseases linked with ones lifestyle. These diseases are non-communicable diseases. They are caused by lack of physical activity, unhealthy eating, alcohol, substance use disorders and smoking tobacco, which can lead to heart disease, stroke, obesity, type II diabetes and Lung cancer. The diseases that appear to increase in frequency as countries become more industrialized and people live longer include Alzheimer's disease, arthritis, atherosclerosis, asthma, cancer, chronic liver disease or cirrhosis, chronic obstructive pulmonary disease, colitis, irritable bowel syndrome, type 2 diabetes, heart disease, hypertension, metabolic syndrome, chronic kidney failure, osteoporosis, PCOD, stroke, depression, obesity and vascular dementia.

Cardiovascular disease (CVD) is a class of diseases that involve the heart or blood vessels. CVD includes coronary artery diseases (CAD) such as angina and myocardial infarction. Other CVDs include stroke, heart failure, hypertensive heart disease, rheumatic heart disease, cardiomyopathy, abnormal heart rhythms, congenital heart disease, valvular heart disease, carditis, aortic aneurysms, peripheral artery disease, thromboembolic disease, and venous thrombosis.

Chronic kidney disease (CKD) is a type of kidney disease in which there is gradual loss of kidney function over a period of months to years. Initially there are generally no symptoms; later, symptoms may include leg swelling, feeling tired, vomiting, loss of appetite, and confusion. Complications include an increased risk of heart disease, high blood pressure, bone disease, and anemia.

Preventive healthcare, or prophylaxis, consists of measures taken for disease prevention. Disease and disability are affected by environmental factors, genetic predisposition, disease agents, and lifestyle choices, and are dynamic processes which begin before individuals realize they are affected. Disease prevention relies on anticipatory actions that can be categorized as primal, primary, secondary, and tertiary prevention.
Diseases of affluence, previously called diseases of rich people, is a term sometimes given to selected diseases and other health conditions which are commonly thought to be a result of increasing wealth in a society. Also referred to as the "Western disease" paradigm, these diseases are in contrast to so-called "diseases of poverty", which largely result from and contribute to human impoverishment. These diseases of affluence have vastly increased in prevalence since the end of World War II.

A non-communicable disease (NCD) is a disease that is not transmissible directly from one person to another. NCDs include Parkinson's disease, autoimmune diseases, strokes, most heart diseases, most cancers, diabetes, chronic kidney disease, osteoarthritis, osteoporosis, Alzheimer's disease, cataracts, and others. NCDs may be chronic or acute. Most are non-infectious, although there are some non-communicable infectious diseases, such as parasitic diseases in which the parasite's life cycle does not include direct host-to-host transmission.

Health in Ethiopia has improved markedly since the early 2000s, with government leadership playing a key role in mobilizing resources and ensuring that they are used effectively. A central feature of the sector is the priority given to the Health Extension Programme, which delivers cost-effective basic services that enhance equity and provide care to millions of women, men and children. The development and delivery of the Health Extension Program, and its lasting success, is an example of how a low-income country can still improve access to health services with creativity and dedication.

The major causes of deaths in Finland are cardiovascular diseases, malignant tumors, dementia and alzheimers disease, respiratory diseases, alcohol related diseases and accidental poisoning by alcohol. In 2010 the leading causes of death among men aged 15 to 64 were alcohol related deaths, ischaemic heart disease, accident, suicides, lung cancer and cerbrovascular diseases. Among women the leading causes were breast cancer, alcohol related deaths, accidents, suicides, ischaemic heart disease and lung cancer.
The obesity paradox is a medical hypothesis which holds that obesity may, counterintuitively, be protective and associated with greater survival in certain groups of people, such as very elderly individuals or those with certain chronic diseases. It further postulates that normal to low body mass index or normal values of cholesterol may be detrimental and associated with higher mortality in asymptomatic people. The hypothesis is controversial and is disputed by many scientists.
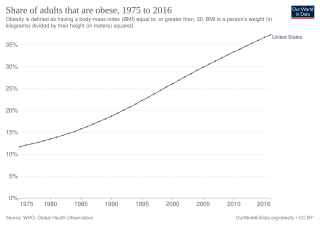
Obesity in the United States is a major health issue resulting in numerous diseases, specifically increased risk of certain types of cancer, coronary artery disease, type 2 diabetes, stroke, cardiovascular disease, as well as significant increases in early mortality and economic costs.

Being overweight or fat is having more body fat than is optimally healthy. Being overweight is especially common where food supplies are plentiful and lifestyles are sedentary.

Obesity in the Middle East and North Africa is a notable health issue. Out of the fifteen fattest nations in the world as of 2014, 5 were located in the Middle East and North Africa region.
Life expectancy in Nicaragua at birth was 72 years for men and 78 for women in 2016. While communicable diseases such as dengue, chikungunya, and Zika continue to persist as national health concerns, there is a rising public health threat of non-communicable diseases such as diabetes, cardiovascular disease, and cancer, which were diseases previously thought to be more relevant and problematic for more developed nations. Additionally, in the women's health sector, high rates of adolescent pregnancy and cervical cancer continue to persist as national concerns.
Lebanon is a small middle-income country on the Eastern Mediterranean shore with a population of around 4 million Lebanese citizens, 1.2 million Syrian refugees, and half a million Palestinian refugees. It is at the third stage of its demographic transition characterized by a decline in both fertility and mortality rates. Moreover, Lebanon, like many countries in the Middle East is experiencing an epidemiological transition with an increasingly ageing population suffering from chronic and non-communicable diseases. Mortality related to non-communicable diseases is 404.4 deaths per 100,000 individuals, with an estimate of 45% due to cardiovascular diseases, making them the leading cause of death in Lebanon. Lebanon has health indices that are close to those of more developed countries, with a reported life expectancy at birth of 80.1 years and an under-five mortality rate of 9.5 per 1,000 live births in 2016. Since the end of the 15-year Lebanese Civil War in 1990, Lebanon’s health indicators have significantly improved.
This article provides a global overview of the current trends and distribution of metabolic syndrome. Metabolic syndrome refers to a cluster of related risk factors for cardiovascular disease that includes abdominal obesity, diabetes, hypertension, and elevated cholesterol.
Montenegro is a country with an area of 13,812 square kilometres and a population of 620,029, according to the 2011 census. The country is bordered by Croatia, the Adriatic Sea, Bosnia, Herzegovina, Serbia, Kosovo and Albania. The most common health issues faced are non-communicable diseases accounting for 95% of all deaths. This is followed by 4% of mortality due to injury, and 1% due to communicable, maternal, perinatal and nutritional conditions. Other health areas of interest are alcohol consumption, which is the most prevalent disease of addiction within Montenegro and smoking. Montenegro has one of the highest tobacco usage rates across Europe. Life expectancy for men is 74 years, and life expectancy for women is 79.
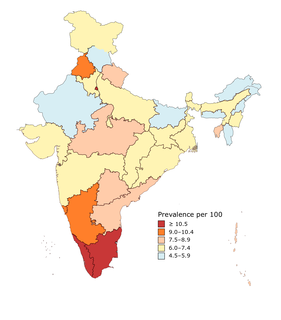
India has an estimated 77 million people with diabetes, which makes it the second most affected in the world, after China. One in six people (17%) in the world with diabetes is from India. The number is projected to grow by 2045 to become 134 million per the International Diabetes Federation.

Cardiovascular disease in women is an integral area of research in the ongoing studies of women's health. Cardiovascular disease (CVD) is an umbrella term for a wide range of diseases affecting the heart and blood vessels, including but not limited to, coronary artery disease (CAD), stroke, cardiomyopathy, and aortic aneurysms.
References
- ↑ Strong K, Mathers C, Leeder S, Beaglehole R. Preventing chronic diseases: how many lives can we save?. Lancet 2005;
- ↑ Nelson R., Cancer Needs to Become a National Priority in China, May 01, 2014, Accessed 5/3/2014
- ↑ Challenges to effective cancer control in China, India, and Russia, The Lancet Oncology, 15(5), 489-538, April 2014, doi:10.1016/S1470-2045(14)70029-4, Accessed 5/3/2014
- 1 2 Fifth National Population Census. Beijing: National Bureau of Statistics of China, 2000.
- 1 2 3 4 5 6 Leeder S, Raymond S, Greenberg H, et al. A race against time: the challenge of cardiovascular disease in developing economies. New York: Columbia University, 2005.
- 1 2 3 4 5 Ministries of Health and Science and Technology and the National Bureau of Statistics of the People's Republic of China. The nutrition and health status of the Chinese people. Beijing: State Information Office, 2004.
- ↑ "Diabetes can shorten lifespan by nine years in Chinese patients". WebMD China. January 18, 2017.
- ↑ Yang G, Ma J, Liu N, Zhou L. Smoking and passive smoking in Chinese. Chin J Epidemiol 2005; 26: 78-83.
- ↑ Yang L, Parkin DM, Li YD, et al. Estimation and projection of the national profile of cancer mortality in China: 1991–2005. Br J Cancer 2004; 90: 2157-2166.
- ↑ Wang Y, Huang Y, Li A, et al. A survey of adolescent smoking and tobacco knowledge in four areas of China. Chin J School Health 2000; 21: 456-457.
- ↑ Ji C, Sun J, Chen T. Dynamic analysis on the prevalence of obesity and overweight school-age children and adolescents in recent 15 years in China. Chin J Epidemiol 2004; 25: 103-104.
- ↑ WHO. Preventing chronic diseases: a vital investment. Geneva: World Health Organization, 2005.
- ↑ Wen C. China's plans to curb cervical cancer. Lancet Oncol 2005; 6: 139-140.
- ↑ Wang WZ, et al. Change of incidence of stroke after a community-based intervention for nine years in three cities in China. Chin J Chron Non-commun Dis 2002; 4: 30-33.
- ↑ Wang WZ, et al. Change of mortality of stroke after a community-based intervention for nine years in three cities in China. Chin J Chron Non-commun Dis 2002; 4: 49-51.
- ↑ The World Bank Loan for China Disease prevention project—Health VII project. Health promotion component. External evaluation report. Geneva: World Bank, 2004.
- 1 2 Armstrong T, Bonita R. Capacity building for integrated noncommunicable disease risk factor surveillance system in developing countries. Ethn Dis 2003; 13: S2-S13.