| Joints of the hand | |
|---|---|
 The DIP, PIP and MCP joints of the hand:
| |
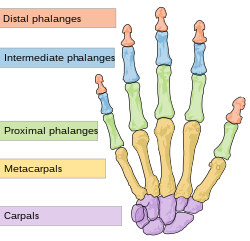 Human hand bones | |
| Details | |
| Identifiers | |
| Latin | articulationes interphalangeae manus, articulationes digitorum manus |
| TA98 | A03.5.11.601 |
| TA2 | 1839 |
| FMA | 35285 |
| Anatomical terminology | |
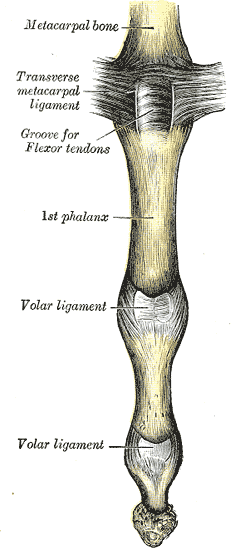
The interphalangeal joints of the hand are the hinge joints between the phalanges of the fingers that provide flexion towards the palm of the hand.
Contents
- Joint structure
- Dorsal structures
- Palmar structures
- Movements
- Clinical significance
- See also
- References
- External links
- Further reading
There are two sets in each finger (except in the thumb, which has only one joint):
- "proximal interphalangeal joints" (PIJ or PIP), those between the first (also called proximal) and second (intermediate) phalanges
- "distal interphalangeal joints" (DIJ or DIP), those between the second (intermediate) and third (distal) phalanges
Anatomically, the proximal and distal interphalangeal joints are very similar. There are some minor differences in how the palmar plates are attached proximally and in the segmentation of the flexor tendon sheath, but the major differences are the smaller dimension and reduced mobility of the distal joint. [1]