
Tuberculosis (TB), also known colloquially as the "white death", or historically as consumption, is an infectious disease usually caused by Mycobacterium tuberculosis (MTB) bacteria. Tuberculosis generally affects the lungs, but it can also affect other parts of the body. Most infections show no symptoms, in which case it is known as latent tuberculosis. Around 10% of latent infections progress to active disease that, if left untreated, kill about half of those affected. Typical symptoms of active TB are chronic cough with blood-containing mucus, fever, night sweats, and weight loss. Infection of other organs can cause a wide range of symptoms.

The Mantoux test or Mendel–Mantoux test is a tool for screening for tuberculosis (TB) and for tuberculosis diagnosis. It is one of the major tuberculin skin tests used around the world, largely replacing multiple-puncture tests such as the tine test. The Heaf test, a form of tine test, was used until 2005 in the UK, when it was replaced by the Mantoux test. The Mantoux test is endorsed by the American Thoracic Society and Centers for Disease Control and Prevention. It was also used in the USSR and is now prevalent in most of the post-Soviet states, although Soviet mantoux produced many false positives due to children's allergic reaction.
Directly observed treatment, short-course is the name given to the tuberculosis (TB) control strategy recommended by the World Health Organization. According to WHO, "The most cost-effective way to stop the spread of TB in communities with a high incidence is by curing it. The best curative method for TB is known as DOTS." DOTS has five main components:

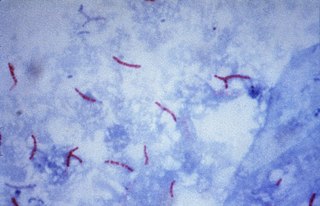
Tuberculosis is diagnosed by finding Mycobacterium tuberculosis bacteria in a clinical specimen taken from the patient. While other investigations may strongly suggest tuberculosis as the diagnosis, they cannot confirm it.

Management of tuberculosis refers to techniques and procedures utilized for treating tuberculosis (TB), or simply a treatment plan for TB.
Tuberculin, also known as purified protein derivative, is a combination of proteins that are used in the diagnosis of tuberculosis. This use is referred to as the tuberculin skin test and is recommended only for those at high risk. Reliable administration of the skin test requires large amounts of training, supervision, and practice. Injection is done into the skin. After 48 to 72 hours, if there is more than a five to ten millimeter area of swelling, the test is considered positive.
Latent tuberculosis (LTB), also called latent tuberculosis infection (LTBI) is when a person is infected with Mycobacterium tuberculosis, but does not have active tuberculosis (TB). Active tuberculosis can be contagious while latent tuberculosis is not, and it is therefore not possible to get TB from someone with latent tuberculosis. The main risk is that approximately 10% of these people will go on to develop active tuberculosis. This is particularly true, and there is added risk, in particular situations such as medication that suppresses the immune system or advancing age.
A health professional, healthcare professional, or healthcare worker is a provider of health care treatment and advice based on formal training and experience. The field includes those who work as a nurse, physician, physician assistant, registered dietitian, veterinarian, veterinary technician, optometrist, pharmacist, pharmacy technician, medical assistant, physical therapist, occupational therapist, dentist, midwife, psychologist, audiologist, or healthcare scientist, or who perform services in allied health professions. Experts in public health and community health are also health professionals.

Mario C. B. Raviglione has been professor at the University of Milan, Italy since March 2018. He directs the activities focused on global health and aiming at pursuing didactic and research in this field as part of the new Multidisciplinary Research in Health Science (MACH) Centre. Part of his activities are devoted to teaching global health principles to undergraduate medical students, making the University of Milan the first in Italy, and one of the pioneers world-wide, introducing global health as a module among the required curricular courses. At the same university, Raviglione is now coordinating the first international Master Course in Global Health in Italy and one of the very few online worldwide . In 2019 and 2020, he was also Professeur Titulaire at the Global Studies Institute (GSI), Université de Genève, Suisse. Through the GSI, he has worked within the context of the Institute of Global Health. Previously, between 2003 and 2017, he was director of the Global Tuberculosis Programme at the World Health Organization (WHO) . He graduated in medicine from the University of Turin in 1980 and then trained in internal medicine and Infectious Diseases at Cabrini Medical Center in New York City and at Beth Israel Medical Center in Boston where he was a Harvard University Clinical Fellow in Medicine and specialised in AIDS. Back in Europe, Raviglione joined WHO in 1991 as a Junior Professional Officer, and spent a few years working on TB and AIDS, TB epidemiology in Europe, and anti-TB drug resistance surveillance and response. In the mid-1990s, he set up both the WHO global drug resistance surveillance project and the WHO global TB surveillance and monitoring systems. Among his major achievements are the contributions to the development of the WHO's DOTS Strategy in 1995, and the direction of the development of both the Stop TB Strategy in 2006 and the End TB Strategy in 2014. During his years at WHO he worked with, and visited, more than 50 countries supporting their TB care, prevention, control and research activities. His research work has resulted in over 350 scientific articles and chapters on the topics of infectious diseases, HIV/AIDS, TB, and global health, including the TB chapters in the last eight editions of Harrison's Principles of Internal Medicine. He is editor of the 3rd and 4th edition of "Tuberculosis - A comprehensive international approach", a multi-author book, and associate editor of other books on public health, infectious diseases and tuberculosis. He directed the team that developed the book “Systematic screening for active tuberculosis – Principles and recommendations”, awarded by the British Medical Association as "Highly Commended Book" for Public Health in 2014. He is among the top 10 most cited authors in the TB field. His h-index is 117 and 94 (Scinapse) and his work has been cited over 63000 times. He is also among the top 25 Italian epidemiological scientists and the top 100 Italian scientists in general. As an expert in TB, he has worked as a teacher or visiting professor at Johns Hopkins University, University of Geneva, University of Modena and Reggio Emilia, and University of Pavia. He has been visiting professor at the University of Brescia and has recently lectured at major universities including Harvard, McGill and Sydney. He participates in a variety of board of directors, scientific and advisory committees, including those of the TB Alliance, Doctors with Africa CUAMM, BE Health Association, International Health Commission of the Missionary Sisters of the Sacred Heart - Cabrini Ministries ,Fondazione 3Bi. and the McGill Global Health Programs International Advisory Board. In 2017-2018 and in 2023 he was member of the Lancet Commission on TB. During 2015-2017 he conceived and co-organised, with WHO and the Russian Federation Ministry of Health, the first Global WHO Ministerial Conference on TB in the Sustainable Development Era, held in Moscow on 16–17 November 2017, and his team worked towards ensuring that TB is raised in the international political agenda through the United Nations General Assembly high-level meeting on TB that was held in 2018. As main Editor, he conceived and coordinated with other global health authorities the publication of a landmark book "Global Health Essentials" part of the Springer series devoted to the UN Sustainable Development Goals (SDGs). This practical manual is a comprehensive book written by an esteemed international panel of over 150 experts from 70 institutions across 30 countries, and provides a succinct yet thorough exploration of key global health challenges, issues, and solutions.
Multidrug-resistant tuberculosis (MDR-TB) is a form of tuberculosis (TB) infection caused by bacteria that are resistant to treatment with at least two of the most powerful first-line anti-TB medications (drugs): isoniazid and rifampicin. Some forms of TB are also resistant to second-line medications, and are called extensively drug-resistant TB (XDR-TB).
The National Tuberculosis Elimination Programme (NTEP), earlier known as the Revised National Tuberculosis Control Programme (RNTCP), is the Public Health initiative of the Government of India that organizes its anti-Tuberculosis efforts. It functions as a flagship component of the National Health Mission (NHM) and provides technical and managerial leadership to anti-tuberculosis activities in the country. As per the National Strategic Plan 2017–25, the program has a vision of achieving a "TB free India",with a strategies under the broad themes of "Prevent, Detect,Treat and Build pillars for universal coverage and social protection". The program provides, various free of cost, quality tuberculosis diagnosis and treatment services across the country through the government health system.
Interferon-gamma release assays (IGRAs) are diagnostic tools for latent tuberculosis infection (LTBI). They are surrogate markers of Mycobacterium tuberculosis infection and indicate a cellular immune response to M. tuberculosis if the latter is present.

Tuberculosis is a serious public health problem in China. China has the world's third largest cases of tuberculosis, but progress in tuberculosis control was slow during the 1990s. Detection of tuberculosis had stagnated at around 30% of the estimated total of new cases, and multidrug-resistant tuberculosis was a major problem. These signs of inadequate tuberculosis control can be linked to a malfunctioning health system. The spread of severe acute respiratory syndrome (SARS) in 2003, brought to light substantial weaknesses in the country's public health system. After the government realized the impact that the SARS outbreak had on the country, they increased leadership in their health department. After the SARS epidemic was brought under control, the government increased its commitment and leadership to tackle public health problems and, among other efforts, increased public health funding, revised laws that concerned the control of infectious diseases, implemented the world's largest internet-based disease reporting system to improve transparency, reach and speed, and started a program to rebuild local public health facilities and national infrastructure.
TB Alert is a charity working to raise awareness about and support effective treatment of the disease tuberculosis in the UK and internationally. It was registered in 1998 and launched on World Tuberculosis Day in 1999 in response to the resurgence of tuberculosis (TB) in the UK and worldwide. It is headquartered in Brighton.
Bethania Hospital is located in Sialkot, Pakistan. It is a medical facility owned by the Roman Catholic Archdiocese of Lahore. The hospital treats 60,000 patients a year, 5,000 of which are TB patients. It has a staff of 130 and occupies an area of 300,000 sq. ft.

Tuberculosis in India is a major health problem, causing about 220,000 deaths every year. In 2020, the Indian government made statements to eliminate tuberculosis from the country by 2025 through its National TB Elimination Program. Interventions in this program include major investment in health care, providing supplemental nutrition credit through the Nikshay Poshan Yojana, organizing a national epidemiological survey for tuberculosis, and organizing a national campaign to tie together the Indian government and private health infrastructure for the goal of eliminating the disease.
Government Hospital of Thoracic Medicine, popularly known as the Tambaram TB Sanatorium, is a major state-owned hospital situated in Chennai, India. The hospital is funded and managed by the state government of Tamil Nadu. It was founded in 1928.
Novosibirsk Tuberculosis Research Institute (NTRI) is a Federal State Budgetary Institution of the Ministry of Health of the Russian Federation and it specializes in the research and treatment of tuberculosis. NTRI provides the organization of TB care to the population in the regions of the Siberian and Far Eastern Federal Districts of Russia.
Zarir Udwadia is an Indian pulmonologist and researcher. His work on drug resistant tuberculosis has led to improvements in India's National Tuberculosis Control Programme. Udwadia was the only Indian invited by the WHO to be part of the TB ‘Guidelines Group’, which formulated the 4th edition of the TB Guidelines, published in 2010. He was also the only doctor to be named among India's best strategists.
Truenat is a chip-based, point-of-care, rapid molecular test for diagnosis of infectious diseases. The technology is based on the Taqman RTPCR chemistry which can be performed on the portable, battery operated Truelab Real Time micro PCR platform. Truenat is developed and manufactured by Goa-based Molbio Diagnostics Private Limited.


