In human anatomy, the abdominal aorta is the largest artery in the abdominal cavity. As part of the aorta, it is a direct continuation of the descending aorta.

In human anatomy, the inferior mesenteric artery (IMA) is the third main branch of the abdominal aorta and arises at the level of L3, supplying the large intestine from the distal transverse colon to the upper part of the anal canal. The regions supplied by the IMA are the descending colon, the sigmoid colon, and part of the rectum.
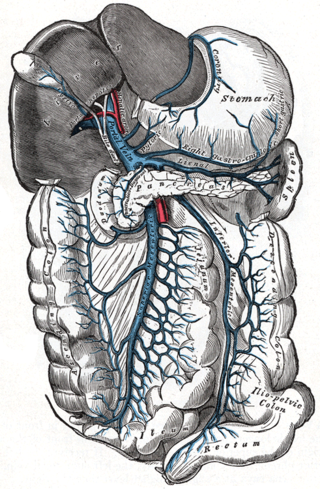
In human anatomy, the inferior mesenteric vein (IMV) is a blood vessel that drains blood from the large intestine. It usually terminates when reaching the splenic vein, which goes on to form the portal vein with the superior mesenteric vein (SMV).

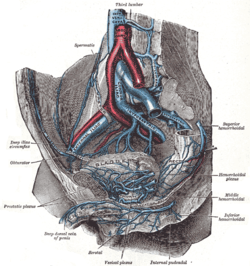
The internal iliac artery is the main artery of the pelvis.

The left colic artery is a branch of the inferior mesenteric artery distributed to the descending colon, and left part of the transverse colon. It ends by dividing into an ascending branch and a descending branch; the terminal branches of the two branches go on to form anastomoses with the middle colic artery, and a sigmoid artery (respectively).

The inferior mesenteric plexus is derived chiefly from the aortic plexus.

The abdominal aortic plexus is formed by branches derived, on either side, from the celiac plexus and ganglia, and receives filaments from some of the lumbar ganglia.

The superior hypogastric plexus is a plexus of nerves situated on the vertebral bodies anterior to the bifurcation of the abdominal aorta. It bifurcates to form the left and the right hypogastric nerve. The SHP is the continuation of the abdominal aortic plexus.

The rectal venous plexus is the venous plexus surrounding the rectum. It consists of an internal and an external rectal plexus. It is drained by the superior, middle, and inferior rectal veins. It forms a portosystemic (portocaval) anastomosis. This allows rectally administered medications to bypass first pass metabolism.
The superior mesenteric plexus is a continuation of the lower part of the celiac plexus, receiving a branch from the junction of the right vagus nerve with the plexus.
The superior rectal artery is an artery that descends into the pelvis to supply blood to the rectum.

The inferior rectal nerves usually branch from the pudendal nerve but occasionally arises directly from the sacral plexus; they cross the ischiorectal fossa along with the inferior rectal artery and veins, toward the anal canal and the lower end of the rectum, and is distributed to the sphincter ani externus and to the integument (skin) around the anus.
The middle rectal veins take origin in the hemorrhoidal plexus and receive tributaries from the bladder, prostate, and seminal vesicle.
The lower part of the external hemorrhoidal plexus is drained by the inferior rectal veins into the internal pudendal vein.

The inferior mesenteric lymph nodes consist of:
The superior rectal plexus supplies the rectum and joins in the pelvis with branches from the pelvic plexuses.

The following outline is provided as an overview of and topical guide to human anatomy:
Transanal hemorrhoidal dearterialization (THD) is a minimally invasive surgical procedure for the treatment of internal hemorrhoids.
Anorectal varices are the dilation of collateral submucosal vessels due to backflow in the veins of the rectum. Typically this occurs due to portal hypertension which shunts venous blood from the portal system through the portosystemic anastomosis present at this site into the systemic venous system. This can also occur in the esophagus, causing esophageal varices, and at the level of the umbilicus, causing caput medusae. Between 44% and 78% of patients with portal hypertension get anorectal varices.