Osteoporosis is a systemic skeletal disorder characterized by low bone mass, micro-architectural deterioration of bone tissue leading to more porous bone, and consequent increase in fracture risk. It is the most common reason for a broken bone among the elderly. Bones that commonly break include the vertebrae in the spine, the bones of the forearm, the wrist, and the hip. Until a broken bone occurs there are typically no symptoms. Bones may weaken to such a degree that a break may occur with minor stress or spontaneously. After the broken bone heals, the person may have chronic pain and a decreased ability to carry out normal activities.

Radiography is an imaging technique using X-rays, gamma rays, or similar ionizing radiation and non-ionizing radiation to view the internal form of an object. Applications of radiography include medical and industrial radiography. Similar techniques are used in airport security,. To create an image in conventional radiography, a beam of X-rays is produced by an X-ray generator and it is projected towards the object. A certain amount of the X-rays or other radiation are absorbed by the object, dependent on the object's density and structural composition. The X-rays that pass through the object are captured behind the object by a detector. The generation of flat two-dimensional images by this technique is called projectional radiography. In computed tomography, an X-ray source and its associated detectors rotate around the subject, which itself moves through the conical X-ray beam produced. Any given point within the subject is crossed from many directions by many different beams at different times. Information regarding the attenuation of these beams is collated and subjected to computation to generate two-dimensional images on three planes which can be further processed to produce a three-dimensional image.

Radiology is the medical specialty that uses medical imaging to diagnose diseases and guide their treatment, within the bodies of humans and other animals. It began with radiography, but today it includes all imaging modalities, including those that use no ionizing electromagnetic radiation, as well as others that do, such as computed tomography (CT), fluoroscopy, and nuclear medicine including positron emission tomography (PET). Interventional radiology is the performance of usually minimally invasive medical procedures with the guidance of imaging technologies such as those mentioned above.
Densitometry is the quantitative measurement of optical density in light-sensitive materials, such as photographic paper or photographic film, due to exposure to light.

Osteopenia, known as "low bone mass" or "low bone density", is a condition in which bone mineral density is low. Because their bones are weaker, people with osteopenia may have a higher risk of fractures, and some people may go on to develop osteoporosis. In 2010, 43 million older adults in the US had osteopenia. Unlike osteoporosis, osteopenia does not usually cause symptoms, and losing bone density in itself does not cause pain.
The body fat percentage (BFP) of a human or other living being is the total mass of fat divided by total body mass, multiplied by 100; body fat includes essential body fat and storage body fat. Essential body fat is necessary to maintain life and reproductive functions. The percentage of essential body fat for women is greater than that for men, due to the demands of childbearing and other hormonal functions. Storage body fat consists of fat accumulation in adipose tissue, part of which protects internal organs in the chest and abdomen. A number of methods are available for determining body fat percentage, such as measurement with calipers or through the use of bioelectrical impedance analysis.
In physical fitness, body composition refers to quantifying the different components of a human body. The selection of compartments varies by model but may include fat, bone, water, and muscle. Two people of the same gender, height, and body weight may have completely different body types as a consequence of having different body compositions. This may be explained by a person having low or high body fat, dense muscles, or big bones.
Bioelectrical impedance analysis (BIA) is a method for estimating body composition, in particular body fat and muscle mass, where a weak electric current flows through the body and the voltage is measured in order to calculate impedance of the body. Most body water is stored in muscle. Therefore, if a person is more muscular there is a high chance that the person will also have more body water, which leads to lower impedance. Since the advent of the first commercially available devices in the mid-1980s the method has become popular owing to its ease of use and portability of the equipment. It is familiar in the consumer market as a simple instrument for estimating body fat. BIA actually determines the electrical impedance, or opposition to the flow of an electric current through body tissues which can then be used to estimate total body water (TBW), which can be used to estimate fat-free body mass and, by difference with body weight, body fat.

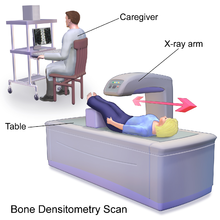
Bone density, or bone mineral density, is the amount of bone mineral in bone tissue. The concept is of mass of mineral per volume of bone, although clinically it is measured by proxy according to optical density per square centimetre of bone surface upon imaging. Bone density measurement is used in clinical medicine as an indirect indicator of osteoporosis and fracture risk. It is measured by a procedure called densitometry, often performed in the radiology or nuclear medicine departments of hospitals or clinics. The measurement is painless and non-invasive and involves low radiation exposure. Measurements are most commonly made over the lumbar spine and over the upper part of the hip. The forearm may be scanned if the hip and lumbar spine are not accessible.

Quantitative computed tomography (QCT) is a medical technique that measures bone mineral density (BMD) using a standard X-ray computed tomography (CT) scanner with a calibration standard to convert Hounsfield units (HU) of the CT image to bone mineral density values. Quantitative CT scans are primarily used to evaluate bone mineral density at the lumbar spine and hip.
Senile osteoporosis has been recently recognized as a geriatric syndrome with a particular pathophysiology. There are different classification of osteoporosis: primary, in which bone loss is a result of aging and secondary, in which bone loss occurs from various clinical and lifestyle factors. Primary, or involuntary osteoporosis, can further be classified into Type I or Type II. Type I refers to postmenopausal osteoporosis and is caused by the deficiency of estrogen. While senile osteoporosis is categorized as an involuntary, Type II, and primary osteoporosis, which affects both men and women over the age of 70 years. It is accompanied by vitamin D deficiency, body's failure to absorb calcium, and increased parathyroid hormone.
Digital X-ray radiogrammetry is a method for measuring bone mineral density (BMD). Digital X-ray radiogrammetry is based on the old technique of radiogrammetry. In DXR, the cortical thickness of the three middle metacarpal bones of the hand is measured in a digital X-ray image. Through a geometrical operation the thickness is converted to bone mineral density. The BMD is corrected for porosity of the bone, estimated by a texture analysis performed on the cortical part of the bone.
Steroid-induced osteoporosis is osteoporosis arising from the use of glucocorticoids analogous to Cushing's syndrome but involving mainly the axial skeleton. The synthetic glucocorticoid prescription drug prednisone is a main candidate after prolonged intake. Bisphosphonates are beneficial in reducing the risk of vertebral fractures. Some professional guidelines recommend prophylactic calcium and vitamin D supplementation in patients who take the equivalent of more than 30 mg hydrocortisone, especially when this is in excess of three months. The use of thiazide diuretics, and gonadal hormone replacement has also been recommended, with the use of calcitonin, bisphosphonates, sodium fluoride or anabolic steroids also suggested in refractory cases. Alternate day use may not prevent this complication.
The trabecular bone score is a measure of bone texture correlated with bone microarchitecture and a marker for the risk of osteoporosis. Introduced in 2008, its main projected use is alongside measures of bone density in better predicting fracture risk in people with metabolic bone problems.
Dual X-ray absorptiometry and laser technique (DXL) in the area of bone density studies for osteoporosis assessment is an improvement to the DXA Technique, adding an exact laser measurement of the thickness of the region scanned. The addition of object thickness adds a third input to the two x-ray energies used by DXA, better solving the equation for bone and excluding more efficiently these soft tissues components.
Single photon absorptiometry is a measuring method for bone density invented by John R. Cameron and James A. Sorenson in 1963.
Ignac Fogelman was a professor of Nuclear Medicine at King’s College London, Honorary Consultant Physician at Guy’s and St Thomas’ NHS Trust, and Director of the Osteoporosis Screening & Research Unit at Guy’s Hospital. He was born in 1948 in Germany and died on 5 July 2016 in the United Kingdom. He is known as the father of bone imaging by some researchers and academics.
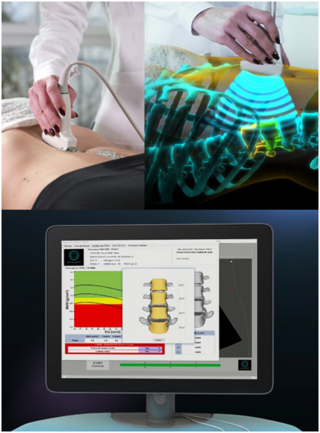
Radiofrequency Echographic Multi Spectrometry (REMS) is a non-ionizing technology for osteoporosis diagnosis and for fracture risk assessment. REMS processes the raw, unfiltered ultrasound signals acquired during an echographic scan of the axial sites, femur and spine. The analysis is performed in the frequency domain. Bone mineral density (BMD) is estimated by comparing the results against reference models.
John A. Shepherd is an American physicist, professor of epidemiology and population sciences and director of the Shepherd Research Laboratory at the University of Hawaii Cancer Center in Honolulu, Hawaii. He is an expert in the use of dual-energy X-ray absorptiometry (DXA) for quantitative bone and soft tissue imaging, and pioneered the use of 3D optical imaging of the whole body for quantifying body composition and associated diseases including cancer risk, obesity, diabetes, and frailty. In 2016, he was the President of the Board of the International Society for Clinical Densitometry.
Catherine Mason Gordon is an American pediatrician who is the Clinical Director of the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health.