Rare,[3] ~0.15 cases per one million per year.[1] 80% age <20 years.[1] M=F[1]
Aneurysmal bone cyst (ABC) is a non-cancerousbone tumor composed of multiple varying sizes of spaces in a bone which are filled with blood.[1][4] The term is a misnomer, as the lesion is neither an aneurysm nor a cyst.[5] It generally presents with pain and swelling in the affected bone.[1] Pressure on neighbouring tissues may cause compression effects such as neurological symptoms.[1]
Treatment is usually by curettage, bone grafting or surgically removing the part of bone.[2] 20–30% may recur, usually in the first couple of years after treatment, particularly in children.[2]
It is rare.[3] The incidence is around 0.15 cases per one million per year.[1] Aneurysmal bone cyst was first described by Jaffe and Lichtenstein in 1942.[5][6]
Signs and symptoms
The afflicted may have relatively small amounts of pain that will quickly increase in severity over a time period of 6–12 weeks. The skin temperature around the bone may increase, a bony swelling may be evident, and movement may be restricted in adjacent joints.[7]
Aneurysmal bone cyst has been widely regarded a reactive process of uncertain cause since its initial description by Jaffe and Lichtenstein in 1942. Many hypotheses have been proposed to explain the cause and pathogenesis of aneurysmal bone cyst, and until very recently the most commonly accepted idea was that aneurysmal bone cyst was the consequence of an increased venous pressure and resultant dilation and rupture of the local vascular network. However, studies by Panoutsakopoulus et al. and Oliveira et al. uncovered the clonal neoplastic nature of aneurysmal bone cyst. Primary cause has been regarded arteriovenous fistula within bone.[9]
They can also be associated with a TRE17/USP6 translocation.[10]
Aneurysmal bone cysts may be intraosseous, staying inside of the bone marrow. Or they may be extraosseous, developing on the surface of the bone, and extending into the marrow. A radiograph will reveal a soap bubble appearance.[citation needed]
Diagnosis
X-ray and CT scan show lytic expansion lesions with clear borders.[1] Expansion of cortex gives the lesion a balloon-like appearance. Larger lesions may appear septated.[11]MRI reveals fluid levels.[1]Bone scan shows outer radiotracer uptake, with a central dark area.[1][11]
Differential diagnosis
Following conditions are excluded before diagnosis can be confirmed:[12]
Unicameral bone cyst
Giant cell tumor
Telangiectatic osteosarcoma
Secondary aneurysmal bone cyst
Treatment
Curettage is performed on some people,[13] and is sufficient for inactive lesions. The recurrence rate with curettage is significant in active lesions, and marginal resection has been advised. Liquid nitrogen, phenol, methyl methacrylate are considered for use to kill cells at margins of resected cyst.[9]
It is rare.[3] The incidence is around 0.15 cases per one million per year.[1] 80% occur in people age less than 20 years.[1] It is second most common tumor of spine and most common benign tumor of pelvis in pediatric population.[9] Males and females are equally affected.[1]
Additional images
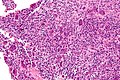
High magnification micrograph of an aneurysmal bone cyst
Intermediate magnification micrograph of an aneurysmal bone cyst
↑ Tomasik, Patryk; Spindel, Jerzy; Miszczyk, Leszek; Chrobok, Adam; Koczy, Bogdan; Widuchowski, Jerzy; Mrozek, Tomasz; Matysiakiewicz, Jacek; Pilecki, Bolesław (September 2009). "Treatment and differential diagnosis of aneurysmal bone cyst based on our own experience". Ortopedia, Traumatologia, Rehabilitacja. 11 (5): 467–475. ISSN1509-3492. PMID19920289.
↑ Zadik, Yehuda; Aktaş Alper; Drucker Scott; Nitzan W Dorrit (2012). "Aneurysmal bone cyst of mandibular condyle: A case report and review of the literature". J Craniomaxillofac Surg. 40 (8): e243–8. doi:10.1016/j.jcms.2011.10.026. PMID22118925.
1 2 Davies, Arthur (2002). Who Manual Of Diagnostic Imaging: Radiographic Anatomy And Interpretation Of The Muskuloskeletal System, VOlume. World Health Organization. pp.168–186. ISBN9241545550.
↑ Differential Diagnosis in Surgical Pathology: Expert Consult - Online and Print, 2e. Elsevier Health Sciences. 2010. pp.878–879. ISBN9781416045809.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.