Related Research Articles

The congenital melanocytic nevus is a type of melanocytic nevus found in infants at birth. This type of birthmark occurs in an estimated 1% of infants worldwide; it is located in the area of the head and neck 15% of the time.
The medical condition pseudopelade of Brocq is a flesh- to pink-colored, irregularly shaped alopecia that may begin in a moth-eaten pattern with eventual coalescence into larger patches of alopecia.
Eccrine angiomatous hamartoma (EAH), first described by Lotzbeck in 1859, is a rare benign vascular hamartoma characterized histologically by a proliferation of eccrine and vascular components. EAH exists on a spectrum of cutaneous tumors that include eccrine nevus, mucinous eccrine nevus and EAH. Each diagnostic subtype is characterized by an increase in the number as well as size of mature eccrine glands or ducts, with EAH being distinguished by the added vascular component.

Acrokeratoelastoidosis of Costa or Acrokeratoelastoidosis is a hereditary form of marginal keratoderma, and can be defined as a palmoplantar keratoderma. It is distinguished by tiny, firm pearly or warty papules on the sides of the hands and, occasionally, the feet. It is less common than the hereditary type of marginal keratoderma, keratoelastoidosis marginalis.
Congenital smooth muscle hamartoma is typically a skin colored or lightly pigmented patch or plaque with hypertrichosis. Congenital smooth muscle hamartoma was originally reported in 1969 by Sourreil et al.

Nevus lipomatosus superficialis is characterized by soft, yellowish papules or cerebriform plaques, usually of the buttock or thigh, less often of the ear or scalp, with a wrinkled rather than warty surface. It is usually congenital in origin or appears within the first three decades.

Solitary mastocytoma, also known as cutaneous mastocytoma, may be present at birth or may develop during the first weeks of life, originating as a brown macule that urticates on stroking. Solitary mastocytoma is a round, erythematous, indurated lesion measuring 1-5 cm in diameter. It can be mildly itchy or asymptomatic and develops over time. Predilection is the head and neck, followed by the trunk, extremities, and flexural areas.
Cutaneous meningioma, also known as heterotopic meningeal tissue, and rudimentary meningocele is a developmental defect, and results from the presence of meningocytes outside the calvarium.
Keratosis pilaris atropicans is a group of idiopathic genodermatoses that consists of three unique clinical entities: atrophoderma vermiculatum, keratosis follicularis spinulosa decalvans, and keratosis pilaris atrophicans faciei.
Hair casts, also known as pseudonits, represent remnants of the inner root sheath, and often occur in great numbers and may mimic nits in the scalp.
Traumatic anserine folliculosis is a curious gooseflesh-like follicular hyperkeratosis that may result from persistent pressure and lateral friction of one skin surface against another. Traumatic anserine folliculosis is caused by trauma. Topical keratolytics are the treatment of choice.
Trichostasis spinulosa is a common but rarely diagnosed disorder of the hair follicles that clinically gives the impression of blackheads, but the follicles are filled with funnel-shaped, horny plugs that are bundles of vellus hairs.
Plica neuropathica, also known as felted hair, is a curling, looping, intertwisting, and felting or matting of the hair in localized areas of the scalp.
Alopecia mucinosa, also known as Follicular mucinosis, Mucinosis follicularis, Pinkus' follicular mucinosis, and Pinkus' follicular mucinosis–benign primary form, is a skin disorder that generally presents, but not exclusively, as erythematous plaques or flat patches without hair primarily on the scalp, neck and face. This can also be present on the body as a follicular mucinosis and may represent a systemic disease.

Annular erythema of infancy(AEI) consists of self-limited eruptions of erythematous, annular to polycyclic patches and plaques. It is an idiopathic figurate erythema. Over several days, a single lesion disappears without leaving behind any scale or hyperpigmentation. Mostly affecting the trunk, face, and extremities, this rash has no symptoms. The diagnosis of AEI is made through a combination of histopathologic and clinical examinations. The disease first manifests in infancy, and if treatment is not received, the periodic eruptions usually stop after the first year of life.
Generalized eruptive histiocytoma is a rare cutaneous condition characterized by widespread, erythematous, essentially symmetrical papules, particularly involving the trunk and proximal extremities.

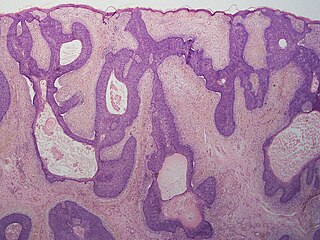
A pilar sheath acanthoma is a cutaneous condition most often found on the face, particularly above the upper lip in adults. Pilar sheath acanthoma is a skin-colored, 5-10 mm diameter papule or nodule with a keratin-filled pore in the center. Pilar sheath acanthoma diagnosis confirmed by shave or excisional biopsy. Successful treatment requires surgical excision.
Basaloid follicular hamartoma is a cutaneous condition characterized as distinctive benign adnexal tumor that has several described variants. It manifest as small tan or brown coloured papules in the trunk, pubic area, face, scalp, and axilla.

Congenital cartilaginous rest of the neck (CCRN) is a minor and very rare congenital cutaneous condition characterized by branchial arch remnants that are considered to be the cervical variant of accessory tragus. It resembles a rudimentary pinna that in most cases is located in the lower anterior part of the neck.
Porokeratotic eccrine ostial and dermal duct nevus (PEODDN) is a skin lesion that resembles a comedonal nevus, but it occurs on the palms and soles where pilosebaceous follicles are normally absent. It is probably transmitted by paradominant transmission.
References
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- 1 2 3 4 5 6 Grover, Chander; Daulatabad, Deepashree; Tanveer, Nadeem (2017). "Nevoid hypertrichosis in a pre-adolescent girl". Indian Dermatology Online Journal. 8 (2). Medknow: 143–145. doi: 10.4103/2229-5178.202285 . ISSN 2229-5178. PMC 5372441 . PMID 28405561.
- 1 2 Vergani, Raffaella; Betti, Roberto; Martino, Patrizia; Crosti, Carlo (2002). "Giant Nevoid Hypertrichosis in an Iranian Girl". Pediatric Dermatology. 19 (1). Wiley: 64–66. doi:10.1046/j.1525-1470.2002.01970.x. ISSN 0736-8046. PMID 11860575.
- 1 2 3 Chang, Sung Nam; Hong, Chang Eui; Kim, Dong-Kun; Park, Wook Hwa (1997). "A Case of Multiple Nevoid Hypertrichosis". The Journal of Dermatology. 24 (5). Wiley: 337–341. doi:10.1111/j.1346-8138.1997.tb02801.x. ISSN 0385-2407. PMID 9198325.
- 1 2 TE, Dudding; M, Rogers; LG, Roddick; J, Relic; MJ, Edwards (1998). "Nevoid hypertrichosis with multiple patches of hair that underwent almost complete spontaneous resolution". American Journal of Medical Genetics. 79 (3). Am J Med Genet: 195–196. doi:10.1002/(sici)1096-8628(19980923)79:3<195::aid-ajmg8>3.0.co;2-m. ISSN 0148-7299. PMID 9788560 . Retrieved 2024-04-23.
- ↑ Gupta, Lipy; Bharadwaj, Minakshi; Gautam, RamKishan (2011). "Nevoid hypertrichosis: Case report with review of the literature". International Journal of Trichology. 3 (2). Medknow: 115–117. doi: 10.4103/0974-7753.90829 . ISSN 0974-7753. PMC 3250008 . PMID 22223975.
- ↑ Koch, D.; Pratsou, P.; Szczecinska, W.; Lanigan, S.; Abdullah, A. (2013-10-31). "The diverse application of laser hair removal therapy: a tertiary laser unit's experience with less common indications and a literature overview". Lasers in Medical Science. 30 (1). Springer Science and Business Media LLC: 453–467. doi:10.1007/s10103-013-1464-5. ISSN 0268-8921. PMID 24173910.