
Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.

A cyst, also traditionally known from Old English as a wen, is a closed sac, having a distinct envelope and division compared with the nearby tissue. Hence, it is a cluster of cells that have grouped together to form a sac ; however, the distinguishing aspect of a cyst is that the cells forming the "shell" of such a sac are distinctly abnormal when compared with all surrounding cells for that given location. A cyst may contain air, fluids, or semi-solid material. A collection of pus is called an abscess, not a cyst. Once formed, a cyst may resolve on its own. When a cyst fails to resolve, it may need to be removed surgically, but that would depend upon its type and location.

A ganglion cyst is a fluid-filled bump associated with a joint or tendon sheath. It most often occurs at the back of the wrist, followed by the front of the wrist.

Pilonidal disease is a type of skin infection which typically occurs as a cyst between the cheeks of the buttocks and often at the upper end. Symptoms may include pain, swelling, and redness. There may also be drainage of fluid, but rarely a fever.

A Bartholin's cyst occurs when a Bartholin's gland within the labia becomes blocked. Small cysts may result in minimal or no symptoms. Larger cysts may result in swelling on one side of the vaginal opening, as well as pain during sex or walking. If the cyst becomes infected, an abscess can occur, which is typically red and very painful. If there are no symptoms, no treatment is needed. Bartholin's cysts affect about 2% of women at some point in their life. They most commonly occur during childbearing years.

A sebaceous gland, or oil gland, is a microscopic exocrine gland in the skin that opens into a hair follicle to secrete an oily or waxy matter, called sebum, which lubricates the hair and skin of mammals. In humans, sebaceous glands occur in the greatest number on the face and scalp, but also on all parts of the skin except the palms of the hands and soles of the feet. In the eyelids, meibomian glands, also called tarsal glands, are a type of sebaceous gland that secrete a special type of sebum into tears. Surrounding the female nipple, areolar glands are specialized sebaceous glands for lubricating the nipple. Fordyce spots are benign, visible, sebaceous glands found usually on the lips, gums and inner cheeks, and genitals.

A dermoid cyst is a teratoma of a cystic nature that contains an array of developmentally mature, solid tissues. It frequently consists of skin, hair follicles, and sweat glands, while other commonly found components include clumps of long hair, pockets of sebum, blood, fat, bone, nail, teeth, eyes, cartilage, and thyroid tissue.

A thyroglossal cyst is a fibrous cyst that forms from a persistent thyroglossal duct. Thyroglossal cysts can be defined as an irregular neck mass or a lump which develops from cells and tissues left over after the formation of the thyroid gland during developmental stages.

A chalazion or meibomian cyst is a cyst in the eyelid usually due to a blocked meibomian gland, typically in the middle of the eyelid, red, and not painful. They tend to come on gradually over a few weeks.

An epidermoid cyst or epidermal inclusion cyst is a benign cyst usually found on the skin. The cyst develops out of ectodermal tissue. Histologically, it is made of a thin layer of squamous epithelium.

Pelvic exenteration is a radical surgical treatment that removes all organs from a person's pelvic cavity. It is used to treat certain advanced or recurrent cancers. The urinary bladder, urethra, rectum, and anus are removed. In women, the vagina, cervix, uterus, Fallopian tubes, ovaries and, in some cases, the vulva are removed. In men, the prostate is removed. The procedure leaves the person with a permanent colostomy and urinary diversion.

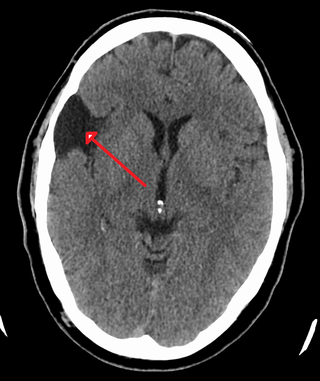
A colloid cyst is a non-malignant tumor in the brain. It consists of a gelatinous material contained within a membrane of epithelial tissue. It is almost always found just posterior to the foramen of Monro in the anterior aspect of the third ventricle, originating from the roof of the ventricle. Because of its location, it can cause obstructive hydrocephalus and increased intracranial pressure. Colloid cysts represent 0.5–1.0% of intracranial tumors.

A trichilemmal cyst is a common cyst that forms from a hair follicle, most often on the scalp, and is smooth, mobile, and filled with keratin, a protein component found in hair, nails, skin, and horns. Trichilemmal cysts are clinically and histologically distinct from trichilemmal horns, hard tissue that is much rarer and not limited to the scalp. Rarely, these cysts may grow more extensively and form rapidly multiplying trichilemmal tumors, also called proliferating trichilemmal cysts, which are benign, but may grow aggressively at the cyst site. Very rarely, trichilemmal cysts can become cancerous.

Skin biopsy is a biopsy technique in which a skin lesion is removed to be sent to a pathologist to render a microscopic diagnosis. It is usually done under local anesthetic in a physician's office, and results are often available in 4 to 10 days. It is commonly performed by dermatologists. Skin biopsies are also done by family physicians, internists, surgeons, and other specialties. However, performed incorrectly, and without appropriate clinical information, a pathologist's interpretation of a skin biopsy can be severely limited, and therefore doctors and patients may forgo traditional biopsy techniques and instead choose Mohs surgery.

Steatocystoma multiplex, is a benign, autosomal dominant congenital condition resulting in multiple cysts on a person's body. Steatocystoma simplex is the solitary counterpart to steatocystoma multiplex.
Eruptive vellus hair cysts are small lesions that occur most often in the chest wall, abdomen and extremities, often with a crusted surface. EVHC may occur randomly, or it can be inherited as an autosomal dominant trait; sporadic cases usually appear at 4–18 years of age. The cysts appear similar clinically to steatocystoma multiplex, as well as acneiform eruptions and milia. Histopathology is the basis of diagnosis. Retinoids, surgery, and lasers are used as treatment modalities.
A central nervous system cyst is a type of cyst that presents and affects part of the central nervous system (CNS). They are usually benign and filled with either cerebrospinal fluid, blood, or tumor cells. CNS cysts are classified into two categories: cysts that originate from non-central nervous system tissue, migrate to, and form on a portion of the CNS, and cysts that originate within central nervous system tissue itself. Within these two categories, there are many types of CNS cysts that have been identified from previous studies.

A breast mass, also known as a breast lump, is a localized swelling that feels different from the surrounding tissue. Breast pain, nipple discharge, or skin changes may be present. Concerning findings include masses that are hard, do not move easily, are of an irregular shape, or are firmly attached to surrounding tissue.

Intracranial epidermoid cysts develop in the early embryonic phases. The cysts develop when epithelial cells are confined with cells that form the brain.

Vaginal cysts are uncommon benign cysts that develop in the vaginal wall. The type of epithelial tissue lining a cyst is used to classify these growths. They can be congenital. They can present in childhood and adulthood. The most common type is the squamous inclusion cyst. It develops within vaginal tissue present at the site of an episiotomy or other vaginal surgical sites. In most instances they do not cause symptoms and present with few or no complications. A vaginal cyst can develop on the surface of the vaginal epithelium or in deeper layers. Often, they are found by the woman herself and as an incidental finding during a routine pelvic examination. Vaginal cysts can mimic other structures that protrude from the vagina such as a rectocele and cystocele. Some cysts can be distinguished visually but most will need a biopsy to determine the type. Vaginal cysts can vary in size and can grow as large as 7 cm. Other cysts can be present on the vaginal wall though mostly these can be differentiated. Vaginal cysts can often be palpated (felt) by a clinician. Vaginal cysts are one type of vaginal mass, others include cancers and tumors. The prevalence of vaginal cysts is uncertain since many go unreported but it is estimated that 1 out of 200 women have a vaginal cyst. Vaginal cysts may initially be discovered during pregnancy and childbirth. These are then treated to provide an unobstructed delivery of the infant. Growths that originate from the urethra and other tissue can present as cysts of the vagina.


