This article may be too technical for most readers to understand.(March 2025) |
| Nutcracker syndrome | |
|---|---|
| Other names | Nutcracker phenomenon, renal vein entrapment syndrome, mesoaortic compression of the left renal vein |
 | |
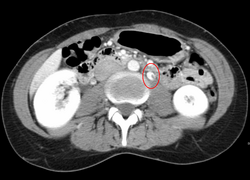
| The nutcracker syndrome results from compression of the left renal vein between the aorta and the superior mesenteric artery. | |
The nutcracker syndrome (NCS) results most commonly from the compression of the left renal vein (LRV) between the abdominal aorta (AA) and superior mesenteric artery (SMA), although other variants exist. [1] [2] The name derives from the fact that, in the sagittal plane and/or transverse plane, the SMA and AA (with some imagination) appear to be a nutcracker crushing a nut (the renal vein).
Contents
- Signs and symptoms
- Cause
- Diagnosis
- Doppler Ultrasound
- CT and MRI
- Venography
- Differential diagnosis
- Treatment
- Conservative management
- Surgical management
- Post-Procedure Follow-Up
- Gallery
- References
- External links
There is a wide spectrum of clinical presentations and diagnostic criteria are not well defined, which frequently results in delayed or incorrect diagnosis. [1] The first clinical report of Nutcracker phenomenon appeared in 1950. [3]
This condition is not to be confused with superior mesenteric artery syndrome, which is the compression of the third portion of the duodenum by the SMA and the AA.