
Migraine is a genetically influenced complex neurological disorder characterized by episodes of moderate-to-severe headache, most often unilateral and generally associated with nausea and light and sound sensitivity. Other characterizing symptoms may include nausea, vomiting, cognitive dysfunction, allodynia, and dizziness. Exacerbation of headache symptoms during physical activity is another distinguishing feature. Up to one-third of migraine sufferers experience aura: a premonitory period of sensory disturbance widely accepted to be caused by cortical spreading depression at the onset of a migraine attack. Although primarily considered to be a headache disorder, migraine is highly heterogenous in its clinical presentation and is better thought of as a spectrum disease rather than a distinct clinical entity. Disease burden can range from episodic discrete attacks, consisting of as little as several lifetime attacks, to chronic disease.

Headache, also known as cephalalgia, is the symptom of pain in the face, head, or neck. It can occur as a migraine, tension-type headache, or cluster headache. There is an increased risk of depression in those with severe headaches.
Cluster headache (CH) is a neurological disorder characterized by recurrent severe headaches on one side of the head, typically around the eye(s). There is often accompanying eye watering, nasal congestion, or swelling around the eye on the affected side. These symptoms typically last 15 minutes to 3 hours. Attacks often occur in clusters which typically last for weeks or months and occasionally more than a year.

Tension headache, stress headache, or tension-type headache (TTH), is the most common type of primary headache. The pain usually radiates from the lower back of the head, the neck, eyes or other muscle groups in the body typically affecting both sides of the head. Tension-type headaches account for nearly 90% of all headaches.
A medication overuse headache (MOH), also known as a rebound headache, usually occurs when painkillers are taken frequently to relieve headaches. These cases are often referred to as painkiller headaches. Rebound headaches frequently occur daily, can be very painful and are a common cause of chronic daily headache. They typically occur in patients with an underlying headache disorder such as migraine or tension-type headache that "transforms" over time from an episodic condition to chronic daily headache due to excessive intake of acute headache relief medications. MOH is a serious, disabling and well-characterized disorder, which represents a worldwide problem and is now considered the third-most prevalent type of headache. The proportion of patients in the population with Chronic Daily Headache (CDH) who overuse acute medications ranges from 18% to 33%. The prevalence of medication overuse headache (MOH) varies depending on the population studied and diagnostic criteria used. However, it is estimated that MOH affects approximately 1-2% of the general population, but its relative frequency is much higher in secondary and tertiary care.
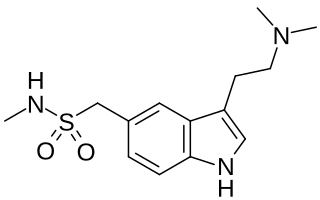
Sumatriptan, sold under the brand name Imitrex among others, is a medication used to treat migraine headaches and cluster headaches. It is taken orally, intranasally, or by subcutaneous injection. Therapeutic effects generally occur within three hours.
Triptans are a family of tryptamine-based drugs used as abortive medication in the treatment of migraines and cluster headaches. This drug class was first commercially introduced in the 1990s. While effective at treating individual headaches, they do not provide preventive treatment and are not considered a cure. They are not effective for the treatment of tension–type headache, except in persons who also experience migraines. Triptans do not relieve other kinds of pain.

Butalbital is a barbiturate with an intermediate duration of action. Butalbital is often combined with other medications, such as paracetamol (acetaminophen) or aspirin, for the treatment of pain and headache. The various formulations combined with codeine are FDA-approved for the treatment of tension headaches. Butalbital has the same chemical formula as talbutal but a different structure—one that presents as 5-allyl-5-isobutylbarbituric acid.
Sexual headache is a type of headache that occurs in the skull and neck during sexual activity, including masturbation or orgasm. These headaches are usually benign, but occasionally are caused by intracranial hemorrhage and cerebral infarction, especially if the pain is sudden and severe. They may be caused by general exertion, sexual excitement, or contraction of the neck and facial muscles. Most cases can be successfully treated with medication.
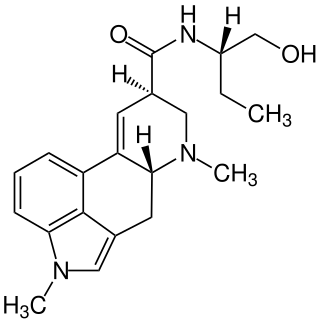
Methysergide, sold under the brand names Deseril and Sansert, is a monoaminergic medication of the ergoline and lysergamide groups which is used in the prophylaxis and treatment of migraine and cluster headaches. It has been withdrawn from the market in the United States and Canada due to adverse effects. It is taken by mouth.
Hemicrania continua (HC) is a persistent unilateral headache that responds to indomethacin. It is usually unremitting, but rare cases of remission have been documented. Hemicrania continua is considered a primary headache disorder, meaning that another condition does not cause it.

Antimigraine drugs are medications intended to reduce the effects or intensity of migraine headache. They include drugs for the treatment of acute migraine symptoms as well as drugs for the prevention of migraine attacks.

Naratriptan (trade names include Amerge) is a triptan drug marketed by GlaxoSmithKline and is used for the treatment of migraine headaches. It is a selective 5-HT1 receptor subtype agonist.
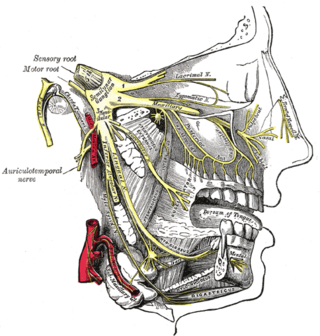
Migraine surgery is a surgical operation undertaken with the goal of reducing or preventing migraines. Migraine surgery most often refers to surgical nerve decompression of one or several nerves in the head and neck which have been shown to trigger migraine symptoms in many migraine sufferers. Following the development of nerve decompression techniques for the relief of migraine pain in the year 2000, these procedures have been extensively studied and shown to be effective in appropriate candidates. The nerves that are most often addressed in migraine surgery are found outside of the skull, in the face and neck, and include the supra-orbital and supra-trochlear nerves in the forehead, the zygomaticotemporal nerve and auriculotemporal nerves in the temple region, and the greater occipital, lesser occipital, and third occipital nerves in the back of the neck. Nerve impingement in the nasal cavity has additionally been shown to be a trigger of migraine symptoms.
Paracetamol/metoclopramide hydrochloride is an oral fixed dose combination prescription medication containing the analgesic paracetamol (500 mg) and the anti-emetic metoclopramide hydrochloride (5 mg). Formulated as a tablet and as sachets of a water-soluble powder, it is sold under the trade name Paramax by Sanofi-Synthelabo, and in Switzerland as Migraeflux MCP, in Australia it is sold as Meteclomax and Anagraine.
Chronic headache, or chronic daily headache (CDH), is classified as experiencing fifteen or more days with a headache per month. It is estimated that chronic headaches affect "4% to 5% of the general population". Chronic headaches consist of different sub-groups, primarily categorized as chronic tension-type headaches and chronic migraine headaches. The treatments for chronic headache are vast and varied. Medicinal and non-medicinal methods exist to help patients cope with chronic headache, because chronic headaches cannot be cured. Whether pharmacological or not, treatment plans are often created on an individual basis. Multiple sources recommend multimodal treatment, which is a combination of medicinal and non-medicinal remedies. Some treatments are controversial and are still being tested for effectiveness. Suggested treatments for chronic headaches include medication, physical therapy, acupuncture, relaxation training, and biofeedback. In addition, dietary alteration and behavioral therapy or psychological therapy are other possible treatments for chronic headaches.
Triptans is a word commonly used for a class of anti-migraine drugs that are selective 5-hydroxytryptamine/serotonin1B/1D (5-HT1B/1D) agonists. Migraine is a complex disease which affects about 15% of the population and can be highly disabling. Triptans have advantages over ergotamine and dihydroergotamine, such as selective pharmacology, well established safety record and evidence-based prescribing instructions. Triptans are therefore often preferred treatment in migraine.
New daily persistent headache (NDPH) is a primary headache syndrome which can mimic chronic migraine and chronic tension-type headache. The headache is daily and unremitting from very soon after onset, usually in a person who does not have a history of a primary headache disorder. The pain can be intermittent, but lasts more than 3 months. Headache onset is abrupt and people often remember the date, circumstance and, occasionally, the time of headache onset. One retrospective study stated that over 80% of patients could state the exact date their headache began.
Preventive treatment of migraine can be an important component of migraine management. Such treatments can take many forms, including everything from surgery, taking certain drugs or nutritional supplements, to lifestyle alterations such as increased exercise and avoidance of migraine triggers.
Occipital nerve stimulation (ONS), also called peripheral nerve stimulation (PNS) of the occipital nerves, is used to treat chronic migraine patients who have failed to respond to pharmaceutical treatments.