A systematic review and network meta-analysis comparing SGLT-2 inhibitors, GLP-1 agonists, and DPP-4 inhibitors demonstrated that use of SGLT2 inhibitors was associated with a 1% reduction in death compared with placebo or no treatment.[7] Another systematic review discussed the mechanisms by which SGLT-2 inhibitors improve cardio-renal function in patients with type 2 diabetes, emphasizing the impacts in improving neural tone.[8]
A meta-analysis including 13 cardiovascular outcome trials found that SGLT-2 inhibitors reduce the risk for three-point major adverse cardiovascular events (MACE), especially in subjects with an estimated glomerular filtration rate (eGFR) below 60 ml/min, whereas GLP-1 receptor agonists were more beneficial in persons with higher eGFR.[9] Likewise, the risk reduction due to SGLT-2 inhibitors was larger in populations with a higher proportion of albuminuria, but this relationship was not observed for GLP-1 receptor agonists. This suggests a differential use of the two substance classes in patients with preserved and reduced renal function or with and without diabetic nephropathy, respectively.[9]
Two reviews have concluded that SGLT2 inhibitors benefit patients with atherosclerotic major adverse cardiovascular events.[10][11] One of those studies defined MACE as the composite of myocardial infarction, stroke, or cardiovascular death.[10]
In May 2015, the FDA issued a warning that gliflozins can increase risk of diabetic ketoacidosis (DKA, a serious condition in which the body produces high levels of blood acids called ketones).[14] By reducing glucose blood circulation, gliflozins cause less stimulation of endogenous insulin secretion or lower dose of exogenous insulin that results in diabetic ketoacidosis. They can specifically cause euglycemic DKA (euDKA, DKA where the blood sugar is not elevated) because of the renal tubular absorption of ketone bodies.[15] A particularly high risk period for ketoacidosis is the perioperative period. SGLT2 inhibitors may need to be discontinued before surgery, and are only recommended when someone is not unwell, is adequately hydrated, and can consume a regular diet.[16] Symptoms of ketoacidosis include nausea, vomiting, abdominal pain, tiredness, and trouble breathing.[17] To lessen the risk of developing ketoacidosis after surgery, the FDA has approved changes to the prescribing information for SGLT2 inhibitor diabetes medicines to recommend they be stopped temporarily before scheduled surgery. Canagliflozin, dapagliflozin, and empagliflozin should each be stopped at least three days before, and ertugliflozin should be stopped at least four days before scheduled surgery.[17]
In September 2015, the FDA issued a warning related to canagliflozin (Invokana) and canagliflozin/metformin (Invokamet) due to decreased bone mineral density and therefore increased risk of bone fractures. Using gliflozins in combination therapy with metformin can lower the risk of hypoglycemia compared to other type 2 diabetes treatments such as sulfonylureas and insulin.[14]
Increased risk of lower limb amputation is associated with canagliflozin, but further data is needed to confirm this risk associated with different gliflozins.[18] A European Medicines Agency review concluded that there is a potential increased risk of lower limb amputation (mostly affecting the toes) in people taking canagliflozin, dapagliflozin and empagliflozin.[19]
In August 2018, the FDA issued a warning of an increased risk of Fournier gangrene in patients using SGLT2 inhibitors.[20] The absolute risk is considered very low.[21]
Interactions are important for SGLT2 inhibitors because most people with type 2 diabetes are taking many other medications. Gliflozins appear to increase the diuretic effect of thiazides, loop diuretics and related diuretics and may increase the risk of dehydration and hypotension.[25] It is important to adjust the dose of antidiabetics if the treatment is combination therapy to avoid hypoglycemia. For example, interactions with sulfonylureas have led to severe hypoglycemia presumably due to cytochrome P450.[26]
Members
Some members of the gliflozin class:
Bexagliflozin was approved in the United States under the brand name Brenzavvy in January 2023.[27]
Canagliflozin is the first SGLT2 inhibitor to be approved for use in the United States. It was approved in March 2013, under the brand name Invokana, and it was also marketed throughout the European Union under the same name.[28][29]
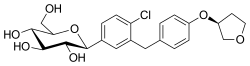
Dapagliflozin (brand name Forxiga) was approved by the EU in 2012, the first SGLT2 inhibitor approved anywhere.[30] It was approved for use in the United States under the brand name Farxiga in January 2014.[31]
Empagliflozin, approved in the United States in August 2014, under the brand name Jardiance by Boehringer Ingelheim.[32] Of the gliflozins, empagliflozin and tofogliflozin have the highest specificity for SGLT2 inhibition.[1] This oral medicine for type 2 diabetes has been shown to reduce the risk of cardiovascular death.[33]
Sotagliflozin (Inpefa) is a dual SGLT1/SGLT2 inhibitor approved by the US Food and Drug Administration (FDA) in May 2023, to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visit in adults with heart failure or type 2 diabetes, chronic kidney disease, and other cardiovascular risk factors.[43][44]
Sodiumglucose cotransporters (SGLTs) are proteins that occur primarily in the kidneys and play an important role in maintaining glucose balance in the blood.[47] SGLT1 and SGLT2 are the two most known SGLTs of this family. SGLT2 is the major transport protein and promotes reabsorption from the glomerular filtration glucose back into circulation and is responsible for approximately 90% of the kidney's glucose reabsorption.[1] SGLT2 is mainly expressed in the kidneys on the epithelial cells lining the first segment of the proximal convoluted tubule. By inhibiting SGLT2, gliflozins prevent the kidneys' reuptake of glucose from the glomerular filtrate and subsequently lower the glucose level in the blood and promote the excretion of glucose in the urine (glucosuria).[48][49]
Reabsorption of glucose in the nephron
The mechanism of action on a cellular level is not well understood. However, it has been shown that binding of different sugars to the glucose site affects the orientation of the aglycone in the access vestibule. So when the aglycone binds, it affects the entire inhibitor. Together, these mechanisms lead to a synergistic interaction. Therefore, variations in the structure of both the sugar and the aglycone are crucial for the pharmacophore of SGLT inhibitors.[50]
Dapagliflozin is an example of an SGLT-2 inhibitor; it is a competitive, highly selective inhibitor of SGLT. It acts via selective and potent inhibition of SGLT-2, and its activity is based on each patient's underlying blood sugar control and kidney function. The results are decreased kidney reabsorption of glucose, glucosuria effect increases with higher levels of glucose in the blood circulation. Therefore, dapagliflozin reduces the blood glucose concentration with a mechanism that is independent of insulin secretion and sensitivity, unlike many other antidiabetic medications. Functional pancreatic β-cells are not necessary for the activity of the medication, so it is convenient for patients with diminished β-cell function.[48][49]
Sodium and glucose are co-transported by the SGLT-2 protein into the tubular epithelial cells across the brush-border membrane of the proximal convoluted tubule. This happens because of the sodium gradient between the tubule and the cell, and therefore provides a secondary active transport of glucose. Glucose is later reabsorbed by the passive transfer of endothelial cells into the interstitial glucose transporter protein.[48][49][51]
In studies that were made on healthy people and people with type 2 diabetes, who were given dapagliflozin in either single ascending dose (SAD) or multiple ascending dose (MAD) showed results that confirmed a pharmacokinetic profile of the medication. With dose-dependent concentrations the half-life is about 12–13 hours, Tmax 1–2 hours and it is protein-bound, so the medication has a rapid absorption and minimal excretion by the kidney.[56]
Dapagliflozin disposition is not evidently affected by body mass index (BMI) or body weight, therefore, the pharmacokinetic findings are expected to be applicable to patients with a higher BMI. Dapagliflozin resulted in dose-dependent increases excretions in urinary glucose, up to 47g/d following single-dose administration, which can be expected from its mechanism of action, dapagliflozin.[57]
Some studies found that dapagliflozin is associated with a decrease in body weight, which is statistically superior compared to placebo or other active comparators.[57][51] It is primarily associated with caloric rather than fluid loss.[57][51]
The most commonly used gliflozins are dapagliflozin, empagliflozin, and canagliflozin. The differences in the structures are relatively small. The general structure includes a glucose sugar with an aromatic group in the β-position at the anomeric carbon. In addition to the glucose sugar moiety and the β-isomeric aryl substituent, the aryl group is composed of a diarylmethylene structure.
The synthesis of gliflozins involves three general steps. The first one is the construction of the aryl substituent, the next one is the introduction of the aryl moiety onto the sugar or glucosylation of the aryl substituent, and the last one is the deprotection and modification of the arylated anomeric center of the sugar.[59]
Phlorizin was the first type of gliflozin, and it was non-selective against SGLT2/SGLT1. It is a natural O-aryl glycoside composed of a d-glucose and an aromatic ketone.[60] However phlorizin is very unstable, it is rapidly degraded by glucosidases in the small intestines, so it can not be used as an orally administrered medication to treat diabetes. Structural modifications have been made to overcome this instability problem. The most efficient way was to conjugate the aryl moiety with the glucose moiety since C-glucosides are more stable in the small intestines than O-glucoside derivatives (C-C bond instead of C-O-C bond).[61]
Phlorizin
In the sugar analogues of dapagliflozin, the β-C series are more active than α-C series so the β-configuration must be at C-1 for the inhibitory activity.[62] Both dapagliflozin and empagliflozin contain a chlorine (Cl) atom in their chemical structure. Cl is a halogen and it has a high electronegativity. This electronegativity withdraws electrons from the bonds, and therefore it reduces the metabolism. The Cl atom also reduces the IC50 value of the medication, so the medication has better activity. The carbon-fluorine bond (C-F) also has a very low electron density.[62]
DapagliflozinEmpagliflozin
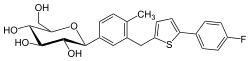
For example, in the chemical structure of canagliflozin, a fluorine atom is connected to an aromatic ring, making the compound more stable and reducing the metabolism of the compound. Empagliflozin contains a tetrahydrofuran ring but not canagliflozin nor dapagliflozin.[63]
Canagliflozin
In the development of gliflozins, the distal ring contains a thiophene ring instead of an aromatic ring. However, the final chemical structures of the marketed gliflozins do not contain this thiophene ring.[64]
SGLT2 inhibitors increase circulating ketone body concentrations.[65] The cardioprotective effects of SGLT2 inhibitors have been attributed to the elevated ketone levels.[66]
Gliflozins have been posited to exhibit protective effects on the heart, liver, kidneys, anti‐hyperlipidemic, anti‐atherosclerotic, anti‐obesity, anti‐neoplastic effects in in vitro, pre‐clinical, and clinical studies. Pleiotropic effects of this class have been attributed to a variety of its pharmacodynamic actions such as natriuresis, hemoconcentration, deactivation of renin-angiotensin-aldosterone system, ketone body formation, alterations in energy homeostasis, glycosuria, lipolysis, anti‐inflammatory, and antioxidative actions.[67][3]
SGLT2 inhibitors have shown beneficial effects on liver function in clinical trials on individuals with NAFLD and type 2 diabetes, and also on those without type 2 diabetes.[68][69]
SGLT2 inhibitors also modified the adverse effects of ozone in heart failure, indicating a potential cardioprotective role.[70]
↑Scheen AJ (2014). "Pharmacodynamics, Efficacy and Safety of Sodium–Glucose Co-Transporter Type2 (SGLT2) Inhibitors for the Treatment of Type2 Diabetes Mellitus". Drugs. 75 (1): 33–59. doi:10.1007/s40265-014-0337-y. PMID25488697. S2CID9350259.
12Zelniker TA, Wiviott SD, abatine MS (2019). "SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials". The Lancet. 393 (10166): 31–39. doi:10.1016/S0140-6736(18)32590-X. PMID30424892. S2CID53277899.
↑Khouri C, Cracowski JL, Roustit M (2018). "SGLT-2 inhibitors and the risk of lower-limb amputation: Is this a class effect?". Diabetes, Obesity and Metabolism. 20 (6): 1531–1534. doi:10.1111/dom.13255. PMID29430814. S2CID3873882.
↑Neuen BL, Young T, Heerspink HJ, Neal B, Perkovic V, Billot L, etal. (November 2019). "SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis". The Lancet. Diabetes & Endocrinology. 7 (11): 845–854. doi:10.1016/S2213-8587(19)30256-6. hdl:10044/1/79694. ISSN2213-8595. PMID31495651. S2CID202003028.
↑Markham, A.J.D., Remogliflozin etabonate: first global approval. 2019. 79(10): p. 1157-1161.
↑Zhang H, Liu J, Zhu X, Li X, Chen H, Wu M, etal. (May 2020). "A Phase I Study on the Pharmacokinetics and Pharmacodynamics of DJT1116PG, a Novel Selective Inhibitor of Sodium-glucose Cotransporter Type 2, in Healthy Individuals at Steady State". Clinical Therapeutics. 42 (5): 892–905.e3. doi:10.1016/j.clinthera.2020.03.007. PMID32265061.
↑"Invokana". drugs.com. Retrieved 31 October 2014.
↑Madaan T, Akhtar M, Najmi AK (2016). "Sodium glucose Co Transporter 2 (SGLT2) inhibitors: Current status and future perspective". European Journal of Pharmaceutical Sciences. 93: 244–252. doi:10.1016/j.ejps.2016.08.025. PMID27531551.
123Yang L, Li H, Li H, Bui A, Chang M, Liu X, etal. (2013). "Pharmacokinetic and Pharmacodynamic Properties of Single- and Multiple-Dose of Dapagliflozin, a Selective Inhibitor of SGLT2, in Healthy Chinese Subjects". Clinical Therapeutics. 35 (8): 1211–1222.e2. doi:10.1016/J.Clinthera.2013.06.017. PMID23910664.
↑LARSON GL (March–April 2015). "The synthesis of gliflozins". Chimica Oggi - Chemistry Today. 33 (2): 37–40. Archived from the original on 30 September 2018. Retrieved 1 October 2018.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.