The human leg, in the general meaning, is the entire lower limb of the human body, including the foot, thigh and even the hip or gluteal region. However, the definition in human anatomy refers only to the section of the lower limb extending from the knee to the ankle, also known as the crus. Legs are used for standing, and all forms of locomotion including recreational such as dancing, and constitute a significant portion of a person's mass. Female legs generally have greater hip anteversion and tibiofemoral angles, but shorter femur and tibial lengths than those in males.
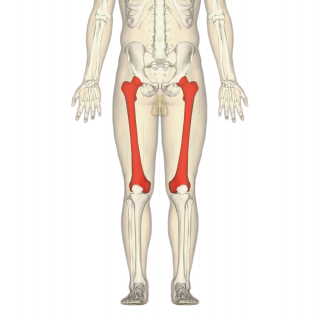
In human anatomy, the thigh is the area between the hip (pelvis) and the knee. Anatomically, it is part of the lower limb.

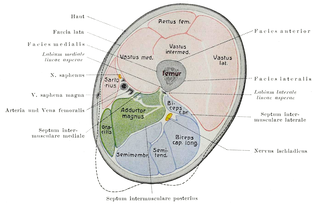
The sartorius muscle is the longest muscle in the human body. It is a long, thin, superficial muscle that runs down the length of the thigh in the anterior compartment.
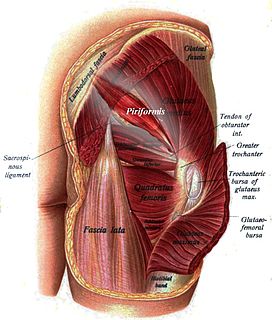
The piriformis is a muscle in the gluteal region of the lower limbs. It is one of the six muscles in the lateral rotator group.

Hip replacement is a surgical procedure in which the hip joint is replaced by a prosthetic implant, that is, a hip prosthesis. Hip replacement surgery can be performed as a total replacement or a hemi (half) replacement. Such joint replacement orthopaedic surgery is generally conducted to relieve arthritis pain or in some hip fractures. A total hip replacement consists of replacing both the acetabulum and the femoral head while hemiarthroplasty generally only replaces the femoral head. Hip replacement is currently one of the most common orthopaedic operations, though patient satisfaction short- and long-term varies widely. Approximately 58% of total hip replacements are estimated to last 25 years. The average cost of a total hip replacement in 2012 was $40,364 in the United States, and about $7,700 to $12,000 in most European countries.
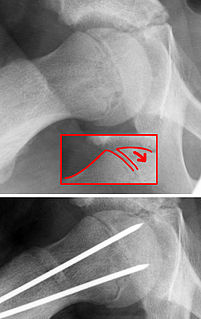
Slipped capital femoral epiphysis is a medical term referring to a fracture through the growth plate (physis), which results in slippage of the overlying end of the femur (metaphysis).

The iliopsoas refers to the joined psoas and the iliacus muscles. The two muscles are separate in the abdomen, but usually merge in the thigh. As such, they are usually given the common name iliopsoas. The iliopsoas muscle joins to the femur at the lesser trochanter, and acts as the strongest flexor of the hip.
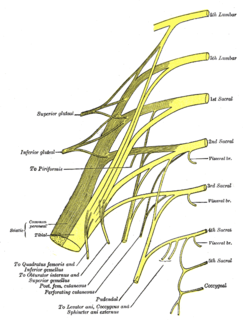
The inferior gluteal nerve is the main motor neuron that innervates the gluteus maximus muscle. It is responsible for the movement of the gluteus maximus in activities requiring the hip to extend the thigh, such as climbing stairs. Injury to this nerve is rare but often occurs as a complication of posterior approach to the hip during hip replacement. When damaged, one would develop gluteus maximus lurch, which is a gait abnormality which causes the individual to 'lurch' backwards to compensate lack in hip extension.
The knee examination, in medicine and physiotherapy, is performed as part of a physical examination, or when a patient presents with knee pain or a history that suggests a pathology of the knee joint.

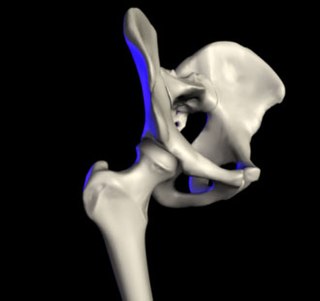
The iliofemoral ligament is a ligament of the hip joint which extends from the ilium to the femur in front of the joint. It is also referred to as the Y-ligament or the ligament of Bigelow, and any combinations of these names.
In medicine, physiotherapy, chiropractic, and osteopathy the hip examination, or hip exam, is undertaken when a patient has a complaint of hip pain and/or signs and/or symptoms suggestive of hip joint pathology. It is a physical examination maneuver.

The acetabular labrum is a ring of cartilage that surrounds the acetabulum of the hip. The anterior portion is most vulnerable when the labrum tears.
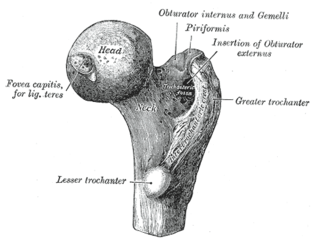
The femur neck is a flattened pyramidal process of bone, connecting the femoral head with the femoral shaft, and forming with the latter a wide angle opening medialward.
The Ortolani test is part of the physical examination for developmental dysplasia of the hip, along with the Barlow maneuver. Specifically, the Ortolani test is positive when a posterior dislocation of the hip is reducible with this maneuver. This is part of the standard infant exam performed preferably in early infancy.

A femoral fracture is a bone fracture that involves the femur. They are typically sustained in high-impact trauma, such as car crashes, due to the large amount of force needed to break the bone. Fractures of the diaphysis, or middle of the femur, are managed differently from those at the head, neck, and trochanter.

Fractures of the acetabulum occur when the head of the femur is driven into the pelvis. This injury is caused by a blow to either the side or front of the knee and often occurs as a dashboard injury accompanied by a fracture of the femur.

The pelvis is either the lower part of the trunk of the human body between the abdomen and the thighs or the skeleton embedded in it.
X-rays of hip dysplasia are one of the two main methods of medical imaging to diagnose hip dysplasia, the other one being medical ultrasonography.. Ultrasound imaging yields better results defining the anatomy until the cartilage is ossified. When the infant is around 3 months old a clear roentgenographic image can be achieved. Unfortunately the time the joint gives a good x-ray image is also the point at which nonsurgical treatment methods cease to give good results.