Related Research Articles

The larynx, commonly called the voice box, is an organ in the top of the neck involved in breathing, producing sound and protecting the trachea against food aspiration. The opening of larynx into pharynx known as the laryngeal inlet is about 4–5 centimeters in diameter. The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus. The word 'larynx' comes from the Ancient Greek word lárunx ʻlarynx, gullet, throat.ʼ

Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.
Vocal fold cysts are benign masses of the membranous vocal folds. These cysts are enclosed, sac-like structures that are typically of a yellow or white colour. They occur unilaterally on the midpoint of the medial edge of the vocal folds. They can also form on the upper/superior, surface of the vocal folds. There are two types of vocal fold cysts:
- Sub-epithelial vocal fold cysts- located in the superficial lamina propria of the vocal folds.
- Ligament vocal fold cysts- located within the deeper layers of the lamina propria or on the vocal ligament.

Laryngectomy is the removal of the larynx and separation of the airway from the mouth, nose and esophagus. In a total laryngectomy, the entire larynx is removed. In a partial laryngectomy, only a portion of the larynx is removed. Following the procedure, the person breathes through an opening in the neck known as a stoma. This procedure is usually performed by an ENT surgeon in cases of laryngeal cancer. Many cases of laryngeal cancer are treated with more conservative methods. A laryngectomy is performed when these treatments fail to conserve the larynx or when the cancer has progressed such that normal functioning would be prevented. Laryngectomies are also performed on individuals with other types of head and neck cancer. Less invasive partial laryngectomies, including tracheal shaves and Feminization Laryngoplasty may also be performed on transgender women and other female or non-binary identified individuals to feminize the larynx and/or voice. Post-laryngectomy rehabilitation includes voice restoration, oral feeding and more recently, smell and taste rehabilitation. An individual's quality of life can be affected post-surgery.

The posterior cricoarytenoid muscle is a intrinsic muscle of the larynx. It arises from the cricoid cartilage; it inserts onto the arytenoid cartilage of the same side. It is innervated by the recurrent laryngeal nerve. Each acts to open the vocal folds by pulling the vocal fold of the same side laterally. It participates in the production of sounds.
Chondrolaryngoplasty is a surgical procedure in which the thyroid cartilage is reduced in size by shaving down the cartilage through an incision in the throat, generally to aid those who are uncomfortable with the girth of their Adam's apple.

Laryngeal papillomatosis, also known as recurrent respiratory papillomatosis (RRP) or glottal papillomatosis, is a rare medical condition in which benign tumors (papilloma) form along the aerodigestive tract. There are two variants based on the age of onset: juvenile and adult laryngeal papillomatosis. The tumors are caused by human papillomavirus (HPV) infection of the throat. The tumors may lead to narrowing of the airway, which may cause vocal changes or airway obstruction. Laryngeal papillomatosis is initially diagnosed through indirect laryngoscopy upon observation of growths on the larynx and can be confirmed through a biopsy. Treatment for laryngeal papillomatosis aims to remove the papillomas and limit their recurrence. Due to the recurrent nature of the virus, repeated treatments usually are needed. Laryngeal papillomatosis is primarily treated surgically, though supplemental nonsurgical and/or medical treatments may be considered in some cases. The evolution of laryngeal papillomatosis is highly variable. Though total recovery may be observed, it is often persistent despite treatment. The number of new cases of laryngeal papillomatosis cases is approximately 4.3 cases per 100,000 children and 1.8 cases per 100,000 adults annually.

Laryngomalacia is the most common cause of chronic stridor in infancy, in which the soft, immature cartilage of the upper larynx collapses inward during inhalation, causing airway obstruction. It can also be seen in older patients, especially those with neuromuscular conditions resulting in weakness of the muscles of the throat. However, the infantile form is much more common. Laryngomalacia is one of the most common laryngeal congenital disease in infancy and public education about the signs and symptoms of the disease is lacking.
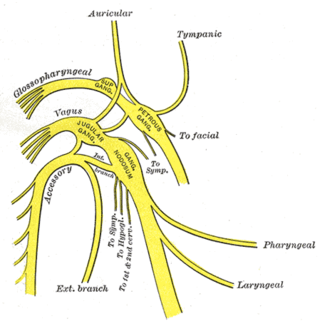
The superior laryngeal nerve is a branch of the vagus nerve. It arises from the middle of the inferior ganglion of vagus nerve and additionally also receives a sympathetic branch from the superior cervical ganglion.

Globus pharyngis, globus hystericus or globus sensation is the persistent but painless sensation of having a pill, food bolus, or some other sort of obstruction in the throat when there is none. Swallowing is typically performed normally, so it is not a true case of dysphagia, but it can become quite irritating. It is common, with 22–45% of people experiencing it at least once in their lifetime.
Vocal cord paresis, also known as recurrent laryngeal nerve paralysis or vocal fold paralysis, is an injury to one or both recurrent laryngeal nerves (RLNs), which control all intrinsic muscles of the larynx except for the cricothyroid muscle. The RLN is important for speaking, breathing and swallowing.
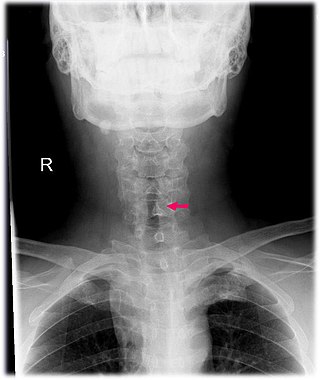
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway. It can be congenital, acquired, iatrogenic, or very rarely, idiopathic. It is defined as the narrowing of the portion of the airway that lies between the vocal cords and the lower part of the cricoid cartilage. In a normal infant, the subglottic airway is 4.5-5.5 millimeters wide, while in a premature infant, the normal width is 3.5 millimeters. Subglottic stenosis is defined as a diameter of under 4 millimeters in an infant. Acquired cases are more common than congenital cases due to prolonged intubation being introduced in the 1960s. It is most frequently caused by certain medical procedures or external trauma, although infections and systemic diseases can also cause it.

Laryngotracheal stenosis refers to abnormal narrowing of the central air passageways. This can occur at the level of the larynx, trachea, carina or main bronchi. In a small number of patients narrowing may be present in more than one anatomical location.

The cricoarytenoid joint is a joint connecting the cricoid cartilage and the arytenoid cartilage. It is a very shallow ball-and-socket joint. It allows for rotation and gliding motion. This controls the abduction and adduction of the vocal cords.

The laryngeal saccules are soft tissue masses that are extensions of the laryngeal ventricles in the larynx. Their function is not well understood, but they may lubricate the vocal cords, and increase the resonance of vocalisation. They may be involved in airway disease and airway obstruction. They may be surgically removed using a laryngeal sacculectomy.
TransOral Robotic Surgery (TORS) is a modern surgical technique used to treat tumors of the mouth and throat via direct access through the mouth. TransOral Robotic Sleep Apnea (TORSA) surgery utilizes the same approach to open the upper airway of patients with obstructive sleep apnea. In TORS and TORSA procedures, the surgeon uses a surgical robot to view and access structures in the oral cavity (mouth) and pharynx (back of the throat) without any incisions through the neck, chin or lip (these incisions are necessary in traditional, non-robotic approaches). Current TORS techniques include radical tonsillectomy, resection of palate and base of skull tumors, hemiglossectomy and resection of tumors above and involving the larynx. The TORSA technique is used for uvulopalatopharyngoplasty, hemiglossectomy, and other airway procedures.
Endoscopic laser cordectomy, also known as Kashima operation, is an endoscopic laser surgical procedure performed for treating the respiratory difficulty caused as a result of bilateral abductor vocal fold paralysis. Bilateral vocal fold paralysis is basically a result of abnormal nerve input to the laryngeal muscles, resulting in weak or total loss of movement of the laryngeal muscles. Most commonly associated nerve is the vagus nerve or in some cases its distal branch, the recurrent laryngeal nerve. Paralysis of the vocal fold may also result from mechanical breakdown of the cricoarytenoid joint. It was first described in by Kashima in 1989.
Arytenoid adduction is a surgical procedure used to treat vocal cord paralysis. A suture is used to emulate the action of the lateral cricoarytenoid muscle and position the paralyzed vocal cord closer to the midline. This allows the two vocal cords to meet and can improve speaking and swallowing ability for affected patients. Arytenoid adduction is often performed in conjunction with medialization thyroplasty.
Laryngotracheal reconstruction is a surgical procedure that involves expanding or removing parts of the airway to widen a narrowing within it, called laryngotracheal stenosis or subglottic stenosis.

Intubation granuloma is a benign growth of granulation tissue in the larynx or trachea, which arises from tissue trauma due to endotracheal intubation. This medical condition is described as a common late complication of tracheal intubation, specifically caused by irritation to the mucosal tissue of the airway during insertion or removal of the patient's intubation tube.
References
- 1 2 3 4 Borkó, R; Szûcs, S (November 2000). "[Congenital laryngeal cysts]". HNO (in German). 48 (11): 843–5. doi:10.1007/s001060050672. PMID 11139891. S2CID 23093039.
- ↑ Burgess, LP; Yim, DW (December 1985). "Laryngeal cyst of the thyroid cartilage". Archives of Otolaryngology. 111 (12): 826. doi:10.1001/archotol.1985.00800140070014. PMID 4062656.
- 1 2 Khashu, M; Osiovich, H; Kozak, F; Pelligra, G; Hirsh, D; Smyth, J (January 2006). "Congenital epiglottic cyst presenting with severe airway obstruction at birth". Journal of Perinatology. 26 (1): 71–72. doi: 10.1038/sj.jp.7211414 . PMID 16355107.
- ↑ Newman, BH; Taxy, JB; Laker, HI (June 1984). "Laryngeal cysts in adults: a clinicopathologic study of 20 cases". American Journal of Clinical Pathology. 81 (6): 715–20. doi:10.1093/ajcp/81.6.715. PMID 6731351.
- ↑ Salerno, G; Mignogna, C; Cavaliere, M; D'Angelo, L; Galli, V (August 2007). "Oncocytic cyst of the larynx: an unusual occurrence". Acta Otorhinolaryngologica Italica. 27 (4): 212–5. PMC 2640029 . PMID 17957853.
- 1 2 NEW, G. B. (1 November 1942). "Treatment of Cysts of the Larynx". Archives of Otolaryngology–Head & Neck Surgery. 36 (5): 687–690. doi:10.1001/archotol.1942.03760050079007.
- ↑ Forte, V; Fuoco, G; James, A (June 2004). "A new classification system for congenital laryngeal cysts". The Laryngoscope. 114 (6): 1123–7. doi:10.1097/00005537-200406000-00031. PMID 15179225. S2CID 7064564.
- ↑ Vocal Fold Cysts Treatment & Management at eMedicine
- ↑ Myssiorek, D; Persky, M (June 1989). "Laser endoscopic treatment of laryngoceles and laryngeal cysts". Otolaryngology–Head and Neck Surgery. 100 (6): 538–41. doi:10.1177/019459988910000602. PMID 2501726. S2CID 28584378.
- ↑ Henderson, LT; Denneny JC, 3rd; Teichgraeber, J (1984). "Airway-obstructing epiglottic cyst". The Annals of Otology, Rhinology, and Laryngology. 94 (5 Pt 1): 473–6. doi:10.1177/000348948509400512. PMID 4051405. S2CID 30724048.
- ↑ DeSanto, LW; Devine, KD; Weiland, LH (January 1970). "Cysts of the larynx—classification". The Laryngoscope. 80 (1): 145–76. doi:10.1288/00005537-197001000-00013. PMID 5411821. S2CID 27525797.