Related Research Articles

A cough is a sudden expulsion of air through the large breathing passages that can help clear them of fluids, irritants, foreign particles and microbes. As a protective reflex, coughing can be repetitive with the cough reflex following three phases: an inhalation, a forced exhalation against a closed glottis, and a violent release of air from the lungs following opening of the glottis, usually accompanied by a distinctive sound.
Shortness of breath (SOB), also known as dyspnea, is a feeling of not being able to breathe well enough. The American Thoracic Society defines it as "a subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity", and recommends evaluating dyspnea by assessing the intensity of the distinct sensations, the degree of distress involved, and its burden or impact on activities of daily living. Distinct sensations include effort/work, chest tightness, and air hunger. The tripod position is often assumed.

Sputum is mucus that is coughed up from the lower airways. In medicine, sputum samples are usually used for naked eye exam, microbiological investigation of respiratory infections and cytological investigations of respiratory systems. It is crucial that the specimen not include any mucoid material from the nose.

Eosinophilia is a condition in which the eosinophil count in the peripheral blood exceeds 5×108/L (500/μL). Hypereosinophilia is an elevation in an individual's circulating blood eosinophil count above 1.5 x 109/L (i.e. 1,500/μL). The hypereosinophilic syndrome is a sustained elevation in this count above 1.5 x 109/L (i.e. 1,500/μL) that is also associated with evidence of eosinophil-based tissue injury.
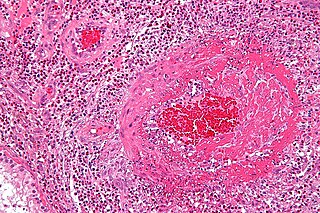
Eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as allergic granulomatosis, is an extremely rare autoimmune condition that causes inflammation of small and medium-sized blood vessels (vasculitis) in persons with a history of airway allergic hypersensitivity (atopy).
Chemical pneumonitis is inflammation of the lung caused by aspirating or inhaling irritants. It is sometimes called a "chemical pneumonia", though it is not infectious. There are two general types of chemical pneumonitis: acute and chronic.

Pneumonitis describes general inflammation of lung tissue. Possible causative agents include radiation therapy of the chest, exposure to medications used during chemo-therapy, the inhalation of debris, aspiration, herbicides or fluorocarbons and some systemic diseases. If unresolved, continued inflammation can result in irreparable damage such as pulmonary fibrosis.

Löffler's syndrome is a disease in which eosinophils accumulate in the lung in response to a parasitic infection. The parasite can be Ascaris, Strongyloides stercoralis, or Dirofilaria immitis which can enter the body through contact with the soil. The symptoms of Löffler's syndrome include those of a parasitic infection such as abdominal pain and cramping, skin rashes and fatigue. Löffler's syndrome itself will cause difficulty breathing, wheeze, coughing as well as a fever.

Respiratory diseases, or lung diseases, are pathological conditions affecting the organs and tissues that make gas exchange difficult in air-breathing animals. They include conditions of the respiratory tract including the trachea, bronchi, bronchioles, alveoli, pleurae, pleural cavity, the nerves and muscles of respiration. Respiratory diseases range from mild and self-limiting, such as the common cold, influenza, and pharyngitis to life-threatening diseases such as bacterial pneumonia, pulmonary embolism, tuberculosis, acute asthma, lung cancer, and severe acute respiratory syndromes, such as COVID-19. Respiratory diseases can be classified in many different ways, including by the organ or tissue involved, by the type and pattern of associated signs and symptoms, or by the cause of the disease.
Acute severe asthma, also known as status asthmaticus, is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators (inhalers) and corticosteroids. Asthma is caused by multiple genes, some having protective effect, with each gene having its own tendency to be influenced by the environment although a genetic link leading to acute severe asthma is still unknown. Symptoms include chest tightness, rapidly progressive dyspnea(shortness of breath), dry cough, use of accessory respiratory muscles, fast and/or labored breathing, and extreme wheezing. It is a life-threatening episode of airway obstruction and is considered a medical emergency. Complications include cardiac and/or respiratory arrest. The increasing prevalence of atopy and asthma remains unexplained but may be due to infection with respiratory viruses.
Pneumonia is an irritation of the lungs caused by different sources. It is characterized by an inflammation of the deep lung tissues and the bronchi. Pneumonia can be acute or chronic. This life-threatening illness is more common in cats than in dogs and the complication “Kennel Cough” can occur in young pets.
Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system to the fungus Aspergillus. It occurs most often in people with asthma or cystic fibrosis. Aspergillus spores are ubiquitous in soil and are commonly found in the sputum of healthy individuals. A. fumigatus is responsible for a spectrum of lung diseases known as aspergilloses.
Loeffler endocarditis is a form of heart disease characterized by a stiffened, poorly-functioning heart caused by infiltration of the heart by white blood cells known as eosinophils. Restrictive cardiomyopathy is a disease of the heart muscle which results in impaired diastolic filling of the heart ventricles, i.e. the large heart chambers which pump blood into the pulmonary or systemic circulation. Diastole is the part of the cardiac contraction-relaxation cycle in which the heart fills with venous blood after the emptying done during its previous systole.
Lungworms are parasitic nematode worms of the order Strongylida that infest the lungs of vertebrates. The name is used for a variety of different groups of nematodes, some of which also have other common names; what they have in common is that they migrate to their hosts' lungs or respiratory tracts, and cause bronchitis or pneumonia. The lungworm will gradually damage the airways or lung tissue by inciting an inflammatory reaction inside the tissue. Ultimately, the parasites survive and reproduce in the respiratory tissues. The category is thus more a descriptive than a precisely taxonomic one.

White blood cells, also called leukocytes or leucocytes, are the cells of the immune system that are involved in protecting the body against both infectious disease and foreign invaders. All white blood cells are produced and derived from multipotent cells in the bone marrow known as hematopoietic stem cells. Leukocytes are found throughout the body, including the blood and lymphatic system.
Eosinophilic bronchitis (EB) is a type of airway inflammation due to excessive mast cell recruitment and activation in the superficial airways as opposed to the smooth muscles of the airways as seen in asthma. It often results in a chronic cough. Lung function tests are usually normal. Inhaled corticosteroids are often an effective treatment.
Tropical (pulmonary) eosinophilia, or TPE, is characterized by coughing, asthmatic attacks, and an enlarged spleen, and is caused by Wuchereria bancrofti, a filarial infection. It occurs most frequently in India and Southeast Asia. Tropical eosinophilia is considered a manifestation of a species of microfilaria. The filariasis is transmitted by a vector, specifically the bite of a Culex, Anopheles, or Aedes mosquito, and the microfilariae (larvae) take up residence in the lung tissue, hindering respiration and causing chest pain as the disease progresses.This disease can be confused with tuberculosis, asthma, or coughs related to roundworms.
Pneumonia can be classified in several ways, most commonly by where it was acquired, but may also by the area of lung affected or by the causative organism. There is also a combined clinical classification, which combines factors such as age, risk factors for certain microorganisms, the presence of underlying lung disease or systemic disease and whether the person has recently been hospitalized.
Eosinophilic myocarditis is inflammation in the heart muscle that is caused by the infiltration and destructive activity of a type of white blood cell, the eosinophil. Typically, the disorder is associated with hypereosinophilia, i.e. an eosinophil blood cell count greater than 1,500 per microliter. It is distinguished from non-eosinophilic myocarditis, which is heart inflammation caused by other types of white blood cells, i.e. lymphocytes and monocytes, as well as the respective descendants of these cells, NK cells and macrophages. This distinction is important because the eosinophil-based disorder is due to a particular set of underlying diseases and its preferred treatments differ from those for non-eosinophilic myocarditis.
Chronic cough is long-term coughing, sometimes defined as more than several weeks or months. The term can be used to describe the different causes related to coughing, the three main ones being upper airway cough syndrome, asthma and gastroesophageal reflux disease. It occurs in the upper airway of the respiratory system. Generally, a cough lasts around one to two weeks; however, chronic cough can persist for an extended period of time defined as six weeks or longer. People with chronic cough often experience more than one cause present. Due to the nature of the syndrome, the treatments used are similar; however, there are a subsequent number of treatments available, and the clinical management of the patients remains a challenge.
References
- ↑ Bain GA, Flower CD (1996). "Pulmonary eosinophilia". European Journal of Radiology. 23 (1): 3–8. doi:10.1016/0720-048X(96)01029-7. PMC 1574763 . PMID 8872069.
- ↑ Research, Center for Drug Evaluation and. "Postmarket Drug Safety Information for Patients and Providers - FDA Drug Safety Communication: Eosinophilic pneumonia associated with the use of Cubicin (daptomycin)". www.fda.gov.
- ↑ Rom WN, Weiden M, Garcia R, et al. (2002). "Acute eosinophilic pneumonia in a New York City firefighter exposed to World Trade Center dust". American Journal of Respiratory and Critical Care Medicine. 166 (6): 797–800. doi:10.1164/rccm.200206-576OC. PMID 12231487.
- ↑ Weller PF (1994). "Parasitic pneumonias". In Pennington, James (ed.). Respiratory infections: diagnosis and management (3rd ed.). New York: Raven Press. p. 695. ISBN 0-7817-0173-2.
- ↑ Jantz MA, Sahn SA (1999). "Corticosteroids in acute respiratory failure". American Journal of Respiratory and Critical Care Medicine. 160 (4): 1079–100. doi:10.1164/ajrccm.160.4.9901075. PMID 10508792.
- ↑ Naughton M, Fahy J, FitzGerald MX (1993). "Chronic eosinophilic pneumonia. A long-term follow-up of 12 patients". Chest. 103 (1): 162–5. doi:10.1378/chest.103.1.162. PMID 8031327.
- ↑ Cottin V, Frognier R, Monnot H, Levy A, DeVuyst P, Cordier JF (2004). "Chronic eosinophilic pneumonia after radiation therapy for breast cancer". European Respiratory Journal. 23 (1): 9–13. doi: 10.1183/09031936.03.00071303 . PMID 14738224.
- ↑ Carrington CB, Addington WW, Goff AM, et al. (1969). "Chronic eosinophilic pneumonia". New England Journal of Medicine. 280 (15): 787–98. doi:10.1056/NEJM196904102801501. PMID 5773637.
- ↑ Badesch DB, King TE, Schwarz MI (1989). "Acute eosinophilic pneumonia: a hypersensitivity phenomenon?". American Review of Respiratory Disease. 139 (1): 249–52. doi:10.1164/ajrccm/139.1.249. PMID 2912347.
- ↑ Allen JN, Pacht ER, Gadek JE, Davis WB (1989). "Acute eosinophilic pneumonia as a reversible cause of noninfectious respiratory failure". New England Journal of Medicine. 321 (9): 569–74. doi:10.1056/NEJM198908313210903. PMID 2761601.