In normal individuals, eosinophils make up about 1–3% of white blood cells, and are about 12–17 micrometres in size with bilobed nuclei.[3][5] While eosinophils are released into the bloodstream, they reside in tissue.[4] They are found in the medulla and the junction between the cortex and medulla of the thymus, and, in the lower gastrointestinal tract, ovaries, uterus, spleen, prostate, and lymph nodes, but not in the skin, lungs, esophagus, or some other internal organs under normal conditions. The presence of eosinophils in these latter organs is associated with disease. For instance, patients with eosinophilic asthma have high levels of eosinophils that lead to inflammation and tissue damage, making it more difficult for patients to breathe.[6][7] Eosinophils persist in the circulation for 8–12 hours, and can survive in tissue for an additional 8–12 days in the absence of stimulation.[8] Pioneering work in the 1980s elucidated that eosinophils were unique granulocytes, having the capacity to survive for extended periods of time after their maturation as demonstrated by ex-vivo culture experiments.[9]
Development
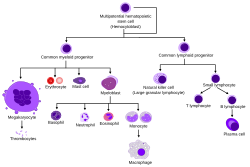
Blood cell lineage
TH2 and ILC2 cells both express the transcription factor GATA-3, which promotes the production of TH2 cytokines, including the interleukins (ILs).[6]IL-5 controls the development of eosinophils in the bone marrow, as they differentiate from myeloid precursor cells.[6][10][11][12] Their lineage fate is determined by transcription factors, including GATA and C/EBP.[3] Eosinophils produce and store many secondary granule proteins prior to their exit from the bone marrow. After maturation, eosinophils circulate in blood and migrate to inflammatory sites in tissues, or to sites of helminth infection in response to chemokines like CCL11 (eotaxin-1), CCL24 (eotaxin-2), CCL5 (RANTES), 5-hydroxyicosatetraenoic acid and 5-oxo-eicosatetraenoic acid, and certain leukotrienes like leukotriene B4 (LTB4) and MCP1/4. Interleukin-13, another TH2 cytokine, primes eosinophilic exit from the bone marrow by lining vessel walls with adhesion molecules such as VCAM-1 and ICAM-1.[6] When eosinophils are activated, they undergo cytolysis, where the breaking of the cell releases eosinophilic granules found in extracellular DNA traps.[6] High concentrations of these DNA traps are known to cause cellular damage, as the granules they contain are responsible for the ligand-induced secretion of eosinophilic toxins which cause structural damage.[6] There is evidence to suggest that eosinophil granule protein expression is regulated by the non-coding RNA EGOT.[13]
Function
Histology of an eosinophil within epithelium, characterized by its bilobed nucleus despite scant visible eosinophilic cytoplasm.
Following activation, eosinophils effector functions include production of the following:
There are also eosinophils that play a role in fighting viral infections, which is evident from the abundance of RNases they contain within their granules, and in fibrin removal during inflammation. Eosinophils, along with basophils and mast cells, are important mediators of allergic responses and asthmapathogenesis and are associated with disease severity. They also fight helminth (worm) colonization and may be slightly elevated in the presence of certain parasites. Eosinophils are also involved in many other biological processes, including postpubertal mammary gland development, oestrus cycling, allograft rejection and neoplasia.[21] They have also been implicated in antigen presentation to T cells.[22]
Eosinophils are responsible for tissue damage and inflammation in many diseases, including asthma.[6][7] High levels of interleukin-5 has been observed to up regulate the expression of adhesion molecules, which then facilitate the adhesion of eosinophils to endothelial cells, thereby causing inflammation and tissue damage.[7]
An accumulation of eosinophils in the nasal mucosa is considered a major diagnostic criterion for allergic rhinitis (nasal allergies).
Granule proteins
Following activation by an immune stimulus, eosinophils degranulate to release an array of cytotoxic granule cationic proteins that are capable of inducing tissue damage and dysfunction.[23] These include:
Strong evidence indicates that blood eosinophil counts can predict the effectiveness of specific anti-inflammatory drugs. Despite their increasing use in clinical practice, data on "normal" blood eosinophil counts remain insufficient. Due to the right-skewed distribution of these counts, median values are more informative than mean values for determining normal levels. Few large-scale studies have reported median blood eosinophil counts, with the median for healthy individuals being 100 cells/μL and the 95th percentile at 420 cells/μL. Thus, it is now evident that the normal median blood eosinophil count in healthy adults is around 100 cells/μL, with counts above 400 cells/μL considered outside the normal range. Current cutoffs such as 150 or 300 cells/μL used in asthma or COPD management fall within the normal range.[29]
Reference ranges for blood tests of white blood cells, comparing eosinophil granulocyte amount (shown in light red) with other cells
Eosinophils play an important role in asthma as the number of accumulated eosinophils corresponds to the severity of asthmatic reaction.[7] Eosinophilia in mice models are shown to be associated with high interleukin-5 levels.[7] Furthermore, mucosal bronchial biopsies conducted on patients with diseases such as asthma have been found to have higher levels of interleukin-5 leading to higher levels of eosinophils.[7] The infiltration of eosinophils at these high concentrations causes an inflammatory reaction.[7] This ultimately leads to airway remodelling and difficulty of breathing.[7]
Eosinophils can also cause tissue damage in the lungs of asthmatic patients.[7] High concentrations of eosinophil major basic protein and eosinophil-derived neurotoxin that approach cytotoxic levels are observed at degranulation sites in the lungs as well as in the asthmatic sputum.[7]
Treatment
Treatments used to combat autoimmune diseases and conditions caused by eosinophils include:
imatinib (STI571) – inhibits PDGF-BB in hypereosinophilic leukemia
Monoclonal antibodies such as dupilumab and lebrikizumab target IL-13 and its receptor, which reduces eosinophilic inflammation in patients with asthma due to lowering the number of adhesion molecules present for eosinophils to bind to, thereby decreasing inflammation.[30][31]Mepolizumab and benralizumab are other treatment options that target the alpha subunit of the IL-5 receptor, thereby inhibiting its function and reducing the number of developing eosinophils as well as the number of eosinophils leading to inflammation through antibody-dependent cell-mediated cytotoxicity and eosinophilic apoptosis.[32][33] Lysosomotropic agents are an efficient means to target the lysosome-like eosinophil granules inducing eosinophil apoptosis.[34]
Animal studies
Within the fat (adipose) tissue of CCR2 deficient mice, there is an increased number of eosinophils, greater alternative macrophage activation, and a propensity towards type 2 cytokine expression. Furthermore, this effect was exaggerated when the mice became obese from a high fat diet.[35]
Mouse models of eosinophilia from mice infected with T. canis showed an increase in IL-5 mRNA in mice spleen.[7]
Mouse models of asthma from OVA show a higher TH2 response.[6] When mice are administered IL-12 to induce the TH1 response, the TH2 response becomes suppressed, showing that mice without TH2 cytokines are significantly less likely to express asthma symptoms.[6]
↑Metcalf D, Begley CG, Nicola NA, Johnson GR (March 1987). "Quantitative responsiveness of murine hemopoietic populations in vitro and in vivo to recombinant multi-CSF (IL-3)". Experimental Hematology. 15 (3): 288–95. PMID3493174.
↑Metcalf D, Burgess AW, Johnson GR, Nicola NA, Nice EC, DeLamarter J, Thatcher DR, Mermod JJ (September 1986). "In vitro actions on hemopoietic cells of recombinant murine GM-CSF purified after production in Escherichia coli: comparison with purified native GM-CSF". Journal of Cellular Physiology. 128 (3): 421–31. doi:10.1002/jcp.1041280311. PMID3528176. S2CID515338.
12Hogan SP, Rosenberg HF, Moqbel R, Phipps S, Foster PS, Lacy P, Kay AB, Rothenberg ME (May 2008). "Eosinophils: biological properties and role in health and disease". Clinical and Experimental Allergy. 38 (5): 709–50. doi:10.1111/j.1365-2222.2008.02958.x. PMID18384431. S2CID25254034.
↑Lacy P (September 2005). "The role of Rho GTPases and SNAREs in mediator release from granulocytes". Pharmacology & Therapeutics. 107 (3): 358–76. doi:10.1016/j.pharmthera.2005.03.008. PMID15951020.
↑Saito K, Nagata M, Kikuchi I, Sakamoto Y (December 2004). "Leukotriene D4 and eosinophil transendothelial migration, superoxide generation, and degranulation via beta2 integrin". Annals of Allergy, Asthma & Immunology. 93 (6): 594–600. doi:10.1016/S1081-1206(10)61269-0. PMID15609771.
↑Kato Y, Fujisawa T, Nishimori H, Katsumata H, Atsuta J, Iguchi K, Kamiya H (2005). "Leukotriene D4 induces production of transforming growth factor-beta1 by eosinophils". International Archives of Allergy and Immunology. 137. 137 Suppl 1 (1): 17–20. doi:10.1159/000085427. PMID15947480. S2CID23556551.
↑Horiuchi T, Weller PF (July 1997). "Expression of vascular endothelial growth factor by human eosinophils: upregulation by granulocyte macrophage colony-stimulating factor and interleukin-5". American Journal of Respiratory Cell and Molecular Biology. 17 (1): 70–7. doi:10.1165/ajrcmb.17.1.2796. PMID9224211.
↑Venge P, Byström J, Carlson M, Hâkansson L, Karawacjzyk M, Peterson C, Sevéus L, Trulson A (September 1999). "Eosinophil cationic protein (ECP): molecular and biological properties and the use of ECP as a marker of eosinophil activation in disease". Clinical and Experimental Allergy. 29 (9): 1172–86. doi:10.1046/j.1365-2222.1999.00542.x. PMID10469025. S2CID11541968.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.




{kind=link}