
The leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. There are 60 bones in each leg.

In humans and other primates, the knee joins the thigh with the leg and consists of two joints: one between the femur and tibia, and one between the femur and patella. It is the largest joint in the human body. The knee is a modified hinge joint, which permits flexion and extension as well as slight internal and external rotation. The knee is vulnerable to injury and to the development of osteoarthritis.

A hamstring is any one of the three posterior thigh muscles in human anatomy between the hip and the knee: from medial to lateral, the semimembranosus, semitendinosus and biceps femoris.

The tibia, also known as the shinbone or shankbone, is the larger, stronger, and anterior (frontal) of the two bones in the leg below the knee in vertebrates ; it connects the knee with the ankle. The tibia is found on the medial side of the leg next to the fibula and closer to the median plane. The tibia is connected to the fibula by the interosseous membrane of leg, forming a type of fibrous joint called a syndesmosis with very little movement. The tibia is named for the flute tibia. It is the second largest bone in the human body, after the femur. The leg bones are the strongest long bones as they support the rest of the body.

The posterior cruciate ligament (PCL) is a ligament in each knee of humans and various other animals. It works as a counterpart to the anterior cruciate ligament (ACL). It connects the posterior intercondylar area of the tibia to the medial condyle of the femur. This configuration allows the PCL to resist forces pushing the tibia posteriorly relative to the femur.
The anterior cruciate ligament (ACL) is one of a pair of cruciate ligaments in the human knee. The two ligaments are called "cruciform" ligaments, as they are arranged in a crossed formation. In the quadruped stifle joint, based on its anatomical position, it is also referred to as the cranial cruciate ligament. The term cruciate is Latin for cross. This name is fitting because the ACL crosses the posterior cruciate ligament to form an "X". It is composed of strong, fibrous material and assists in controlling excessive motion by limiting mobility of the joint. The anterior cruciate ligament is one of the four main ligaments of the knee, providing 85% of the restraining force to anterior tibial displacement at 30 and 90° of knee flexion. The ACL is the most frequently injured ligament in the knee.
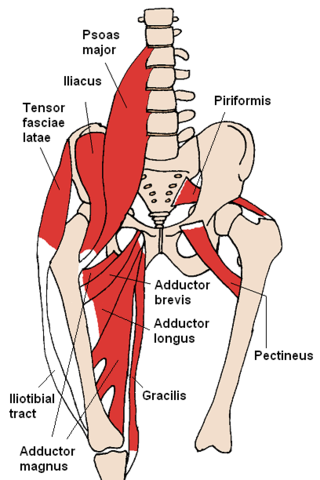
The adductor magnus is a large triangular muscle, situated on the medial side of the thigh.
The gracilis muscle is the most superficial muscle on the medial side of the thigh. It is thin and flattened, broad above, narrow and tapering below.
The semimembranosus muscle is the most medial of the three hamstring muscles in the thigh. It is so named because it has a flat tendon of origin. It lies posteromedially in the thigh, deep to the semitendinosus muscle. It extends the hip joint and flexes the knee joint.

The semitendinosus is a long superficial muscle in the back of the thigh. It is so named because it has a very long tendon of insertion. It lies posteromedially in the thigh, superficial to the semimembranosus.

The medial meniscus is a fibrocartilage semicircular band that spans the knee joint medially, located between the medial condyle of the femur and the medial condyle of the tibia. It is also referred to as the internal semilunar fibrocartilage. The medial meniscus has more of a crescent shape while the lateral meniscus is more circular. The anterior aspects of both menisci are connected by the transverse ligament. It is a common site of injury, especially if the knee is twisted.
The knee examination, in medicine and physiotherapy, is performed as part of a physical examination, or when a patient presents with knee pain or a history that suggests a pathology of the knee joint.
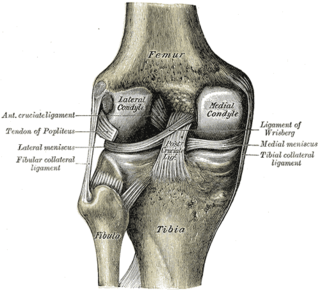
The lateral collateral ligament is an extrinsic ligament of the knee located on the lateral side of the knee. Its superior attachment is at the lateral epicondyle of the femur ; its inferior attachment is at the lateral aspect of the head of fibula. The LCL is not fused with the joint capsule. Inferiorly, the LCL splits the tendon of insertion of the biceps femoris muscle.
An anterior cruciate ligament injury occurs when the anterior cruciate ligament (ACL) is either stretched, partially torn, or completely torn. The most common injury is a complete tear. Symptoms include pain, an audible cracking sound during injury, instability of the knee, and joint swelling. Swelling generally appears within a couple of hours. In approximately 50% of cases, other structures of the knee such as surrounding ligaments, cartilage, or meniscus are damaged.
The unhappy triad, also known as a blown knee among other names, is an injury to the anterior cruciate ligament, medial collateral ligament, and meniscus. Analysis during the 1990s indicated that this 'classic' O'Donoghue triad is actually an unusual clinical entity among athletes with knee injuries. Some authors mistakenly believe that in this type of injury, "combined anterior cruciate and medial collateral ligament disruptions that were incurred during athletic endeavors" always present with concomitant medial meniscus injury. However, the 1990 analysis showed that lateral meniscus tears are more common than medial meniscus tears in conjunction with sprains of the ACL.
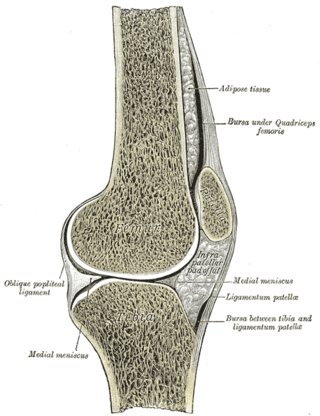
The knee bursae are the fluid-filled sacs and synovial pockets that surround and sometimes communicate with the knee joint cavity. The bursae are thin-walled, and filled with synovial fluid. They represent the weak point of the joint, but also provide enlargements to the joint space. They can be grouped into either communicating and non-communicating bursae or, after their location – frontal, lateral, or medial.

Pellegrini–Stieda syndrome refers to the ossification of the superior part of the medial collateral ligament of the knee. It is a common incidental finding on knee radiographs. It is named for the Italian surgeon A. Pellegrini and the German surgeon A. Stieda (1869–1945). While the eponym is credited to Pellegrini and Stieda, the condition was first discovered by Köhler in 1903, before any namesakes. Pellegrini-Stieda combines the aforementioned radiographic findings and concomitant medial knee joint pain or restricted range of motion.
Posterolateral corner injuries of the knee are injuries to a complex area formed by the interaction of multiple structures. Injuries to the posterolateral corner can be debilitating to the person and require recognition and treatment to avoid long term consequences. Injuries to the PLC often occur in combination with other ligamentous injuries to the knee; most commonly the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). As with any injury, an understanding of the anatomy and functional interactions of the posterolateral corner is important to diagnosing and treating the injury.

A tibial plateau fracture is a break of the upper part of the tibia (shinbone) that involves the knee joint. This could involve the medial, lateral, central, or bicondylar. Symptoms include pain, swelling, and a decreased ability to move the knee. People are generally unable to walk. Complication may include injury to the artery or nerve, arthritis, and compartment syndrome.
Medial knee injuries are the most common type of knee injury. The medial ligament complex of the knee consists of:

