Related Research Articles

Tetralogy of Fallot (TOF), formerly known as Steno-Fallot tetralogy, is a congenital heart defect characterized by four specific cardiac defects. Classically, the four defects are:

Dextrocardia is a rare congenital condition in which the apex of the heart is located on the right side of the body, rather than the more typical placement towards the left. There are two main types of dextrocardia: dextrocardia of embryonic arrest and dextrocardia situs inversus. Dextrocardia situs inversus is further divided.

Situs inversus is a congenital condition in which the major visceral organs are reversed or mirrored from their normal positions. The normal arrangement of internal organs is known as situs solitus. Although cardiac problems are more common, many people with situs inversus have no medical symptoms or complications resulting from the condition, and until the advent of modern medicine, it was usually undiagnosed.
Primary ciliary dyskinesia (PCD) is a rare, autosomal recessive genetic ciliopathy, that causes defects in the action of cilia lining the upper and lower respiratory tract, sinuses, Eustachian tube, middle ear, Fallopian tube, and flagella of sperm cells. The alternative name of "immotile ciliary syndrome" is no longer favored as the cilia do have movement, but are merely inefficient or unsynchronized. When accompanied by situs inversus the condition is known as Kartagener syndrome.

Atrial septal defect (ASD) is a congenital heart defect in which blood flows between the atria of the heart. Some flow is a normal condition both pre-birth and immediately post-birth via the foramen ovale; however, when this does not naturally close after birth it is referred to as a patent (open) foramen ovale (PFO). It is common in patients with a congenital atrial septal aneurysm (ASA).

The jugular venous pressure is the indirectly observed pressure over the venous system via visualization of the internal jugular vein. It can be useful in the differentiation of different forms of heart and lung disease. Classically three upward deflections and two downward deflections have been described.

A ventricular septal defect (VSD) is a defect in the ventricular septum, the wall dividing the left and right ventricles of the heart. The extent of the opening may vary from pin size to complete absence of the ventricular septum, creating one common ventricle. The ventricular septum consists of an inferior muscular and superior membranous portion and is extensively innervated with conducting cardiomyocytes.
The Fontan procedure or Fontan–Kreutzer procedure is a palliative surgical procedure used in children with univentricular hearts. It involves diverting the venous blood from the inferior vena cava (IVC) and superior vena cava (SVC) to the pulmonary arteries without passing through the morphologic right ventricle; i.e., the systemic and pulmonary circulations are placed in series with the functional single ventricle. The procedure was initially performed in 1968 by Francis Fontan and Eugene Baudet from Bordeaux, France, published in 1971, simultaneously described in 1971 by Guillermo Kreutzer from Buenos Aires, Argentina, and finally published in 1973.

Eisenmenger syndrome or Eisenmenger's syndrome is defined as the process in which a long-standing left-to-right cardiac shunt caused by a congenital heart defect causes pulmonary hypertension and eventual reversal of the shunt into a cyanotic right-to-left shunt. Because of the advent of fetal screening with echocardiography early in life, the incidence of heart defects progressing to Eisenmenger syndrome has decreased.

The atrium is one of two upper chambers in the heart that receives blood from the circulatory system. The blood in the atria is pumped into the heart ventricles through the atrioventricular valves.

Transposition of the great vessels (TGV) is a group of congenital heart defects involving an abnormal spatial arrangement of any of the great vessels: superior and/or inferior venae cavae, pulmonary artery, pulmonary veins, and aorta. Congenital heart diseases involving only the primary arteries belong to a sub-group called transposition of the great arteries (TGA), which is considered the most common congenital heart lesion that presents in neonates.

Atrioventricular septal defect (AVSD) or atrioventricular canal defect (AVCD), also known as "common atrioventricular canal" (CAVC) or "endocardial cushion defect" (ECD), is characterized by a deficiency of the atrioventricular septum of the heart that creates connections between all four of its chambers. It is caused by an abnormal or inadequate fusion of the superior and inferior endocardial cushions with the mid portion of the atrial septum and the muscular portion of the ventricular septum.

The Norwood procedure is the first of three surgeries intended to create a new functional systemic circuit in patients with hypoplastic left heart syndrome and other complex heart defects with single ventricle physiology. The first successful Norwood procedure involving the use of a cardiopulmonary bypass was reported by Dr. William Imon Norwood, Jr. and colleagues in 1981.
Cor triatriatum is a congenital heart defect where the left atrium or right atrium is subdivided by a thin membrane, resulting in three atrial chambers.
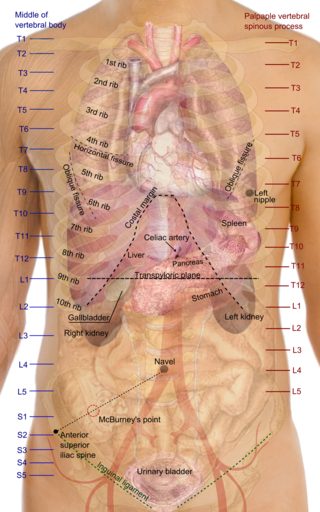
Situs solitus is the medical term referring to the normal position of thoracic and abdominal organs. Anatomically, this means that the heart is on the left with the pulmonary atrium on the right and the systemic atrium on the left along with the cardiac apex. Right-sided organs are the liver, the gall bladder and a trilobed lung as well as the inferior vena cava, while left-sided organs are the stomach, single spleen, a bilobed lung, and the aorta.

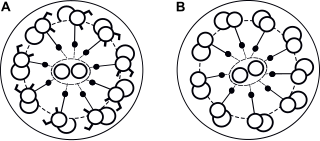
Asplenia with cardiovascular anomalies, also known as Ivemark syndrome and right atrial isomerism, is an example of a heterotaxy syndrome. These uncommon congenital disorders are characterized by defects in the heart, spleen and paired organs such as the lungs and kidneys. Another name is "asplenia-cardiovascular defect-heterotaxy".
Lutembacher's syndrome is a very rare form of congenital heart disease that affects one of the chambers of the heart as well as a valve. It is commonly known as both congenital atrial septal defect (ASD) and acquired mitral stenosis (MS). Congenital atrial septal defect refers to a hole being in the septum or wall that separates the two atria; this condition is usually seen in fetuses and infants. Mitral stenosis refers to mitral valve leaflets sticking to each other making the opening for blood to pass from the atrium to the ventricles very small. With the valve being so small, blood has difficulty passing from the left atrium into the left ventricle. Septal defects that may occur with Lutembacher's syndrome include: Ostium primum atrial septal defect or ostium secundum which is more prevalent.
Polysplenia is a congenital disease manifested by multiple small accessory spleens, rather than a single, full-sized, normal spleen. Polysplenia sometimes occurs alone, but it is often accompanied by other developmental abnormalities. Conditions associated with polysplenia include gastrointestinal abnormalities, such as intestinal malrotation or biliary atresia, as well as cardiac abnormalities, such as dextrocardia.

Arrhythmias, also known as cardiac arrhythmias, heart arrhythmias, or dysrhythmias, are irregularities in the heartbeat, including when it is too fast or too slow. A resting heart rate that is too fast – above 100 beats per minute in adults – is called tachycardia, and a resting heart rate that is too slow – below 60 beats per minute – is called bradycardia. Some types of arrhythmias have no symptoms. Symptoms, when present, may include palpitations or feeling a pause between heartbeats. In more serious cases, there may be lightheadedness, passing out, shortness of breath or chest pain. While most cases of arrhythmia are not serious, some predispose a person to complications such as stroke or heart failure. Others may result in sudden death.
Isolated levocardia is a rare type of organs' situs inversus in which the heart is still in normal position but other abdominal viscera are transposed. Isolated levocardia may occur with heart defects and patients without having operations have low life expectancy: only about 5% to 13% of patients survive more than 5 years. Therefore, even though the risk of cardiac surgeries is high, once patients are diagnosed, operations are suggested to be held as soon as possible. Isolated levocardia is congenital. So far, there is not sufficient evidence to prove that chromosome abnormalities will result in isolated levocardia, and the cause of isolated levocardia is still unknown.
References
- ↑ "heterotaxy syndrome". United States National Library of Medicine . Retrieved 23 May 2016.
- 1 2 3 4 5 6 7 8 9 Lowenthal, A.; et al. (September 26, 2015). "Anatomy, clinical manifestations and diagnosis of heterotaxy (isomerism of the atrial appendages)". Up To Date. Retrieved November 4, 2015.
- ↑ Zhu, Lirong; Belmont, John W.; Ware, Stephanie M. (2005-10-26). "Genetics of human heterotaxias". European Journal of Human Genetics. 14 (1): 17–25. doi: 10.1038/sj.ejhg.5201506 . ISSN 1018-4813. PMID 16251896.
- 1 2 Kim, Soo-Jin (2011). "Heterotaxy Syndrome". Korean Circulation Journal. 41 (5): 227–32. doi:10.4070/kcj.2011.41.5.227. PMC 3116098 . PMID 21731561.
- ↑ Freedom, Robert M.; Treves, S. (1973-05-01). "Splenic Scintigraphy and Radionuclide Venography in the Heterotaxy Syndrome". Radiology. 107 (2): 381–386. doi:10.1148/107.2.381. ISSN 0033-8419. PMID 4695908.
- ↑ Van Praagh, R; et al. (December 15, 1990). "Atrial isomerism in the heterotaxy syndromes with asplenia, or polysplenia, or normally formed spleen: an erroneous concept". Am J Cardiol. 66 (20): 1504–6. doi:10.1016/0002-9149(90)90543-a. PMID 2252000.
- ↑ Cohen, Meryl S.; Anderson, Robert H.; Cohen, Mitchell I.; Atz, Andrew M.; Fogel, Mark; Gruber, Peter J.; Lopez, Leo; Rome, Jonathan J.; Weinberg, Paul M. (2007). "Controversies, genetics, diagnostic assessment, and outcomes relating to the heterotaxy syndrome". Cardiology in the Young. 17 (S2): 29–43. doi:10.1017/s104795110700114x. PMID 18039397. S2CID 206304327.
- ↑ Martínez-Frías ML (March 2001). "Heterotaxia as an outcome of maternal diabetes: an epidemiological study". American Journal of Medical Genetics. 99 (2): 142–6. doi:10.1002/1096-8628(2000)9999:999<00::AID-AJMG1139>3.0.CO;2-Z. PMID 11241474.
- ↑ Maeyama K, Kosaki R, Yoshihashi H, Casey B, Kosaki K (March 2001). "Mutation analysis of left-right axis determining genes in NOD and ICR, strains susceptible to maternal diabetes". Teratology. 63 (3): 119–26. doi:10.1002/tera.1022. PMID 11283968.
- ↑ Kuehl KS, Loffredo C (November 2002). "Risk factors for heart disease associated with abnormal sidedness". Teratology. 66 (5): 242–8. doi:10.1002/tera.10099. PMID 12397632.
- ↑ Kuehl KS, Loffredo CA (March 2003). "Population-based study of l-transposition of the great arteries: possible associations with environmental factors". Birth Defects Research. Part A, Clinical and Molecular Teratology. 67 (3): 162–7. doi:10.1002/bdra.10015. PMID 12797457.
- ↑ Sutherland, Mardi J.; Ware, Stephanie M. (15 November 2009). "Disorders of left-right asymmetry: Heterotaxy and situs inversus". American Journal of Medical Genetics Part C: Seminars in Medical Genetics. 151C (4): 307–317. doi:10.1002/ajmg.c.30228. PMID 19876930. S2CID 23490441.
- ↑ Axelrod, Jeffrey D. (1 February 2020). "Planar cell polarity signaling in the development of left–right asymmetry". Current Opinion in Cell Biology. 62: 61–69. doi:10.1016/j.ceb.2019.09.002. PMC 9258637 . PMID 31654871. S2CID 204918577.
- ↑ Burkhalter MD, Sridhar A, Sampaio P, Jacinto R, Burczyk MS, Donow C, Angenendt M, Competence Network for Congenital Heart Defects Investigators, Hempel M, Walther P, Pennekamp P, Omran H, Lopes SS, Ware SM, Philipp M (2019). "Imbalanced mitochondrial function provokes heterotaxy via aberrant ciliogenesis". J Clin Invest. 129 (7): 2841–2855. doi:10.1172/JCI98890. PMC 6597216 . PMID 31094706.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Chen, CM; et al. (April 2010). "Transcriptional Control of Left–Right Patterning in Cardiac Development". Pediatric Cardiology. 31 (3): 371–377. doi:10.1007/s00246-009-9610-3. PMID 20054532. S2CID 300003.
- ↑ Kosaki, K; Bassi, M T; Kosaki, R; Lewin, M; Belmont, J; Schauer, G; Casey, B (1999-03-01). "Characterization and mutation analysis of human LEFTY A and LEFTY B, homologues of murine genes implicated in left-right axis development". American Journal of Human Genetics. 64 (3): 712–721. doi:10.1086/302289. ISSN 0002-9297. PMC 1377788 . PMID 10053005.
- ↑ Mohapatra, Bhagyalaxmi; Casey, Brett; Li, Hua; Ho-Dawson, Trang; Smith, Liana; Fernbach, Susan D.; Molinari, Laura; Niesh, Stephen R.; Jefferies, John Lynn (2009-03-01). "Identification and functional characterization of NODAL rare variants in heterotaxy and isolated cardiovascular malformations". Human Molecular Genetics. 18 (5): 861–871. doi:10.1093/hmg/ddn411. ISSN 1460-2083. PMC 2722226 . PMID 19064609.
- ↑ Gebbia, Marinella; Ferrero, Giovanni B.; Pilia, Giuseppe; Bassi, Maria T.; Aylsworth, Arthur S.; Penman-Splitt, Miranda; Bird, Lynne M.; Bamforth, John S.; Burn, John (1997-11-01). "X-linked situs abnormalities result from mutations in ZIC3". Nature Genetics. 17 (3): 305–308. doi:10.1038/ng1197-305. PMID 9354794. S2CID 22916101.
- ↑ Applegate, Kimberly E.; Goske, Marilyn J.; Pierce, Gregory; Murphy, Daniel (1999-07-01). "Situs Revisited: Imaging of the Heterotaxy Syndrome". RadioGraphics. 19 (4): 837–852. doi: 10.1148/radiographics.19.4.g99jl31837 . ISSN 0271-5333. PMID 10464794.
- ↑ Lowenthal, Alexander; et al. (October 27, 2015). "Management and outcome of heterotaxy (isomerism of the atrial appendages)". UpToDate. Retrieved December 8, 2015.
- ↑ Brandt, Mary; et al. (October 24, 2015). "Intestinal Malrotation". UpToDate. Retrieved December 10, 2015.
- ↑ Erlichman, Jessi; et al. (August 3, 2015). "Biliary Atresia". UpToDate. Retrieved December 9, 2015.
- ↑ Pasternack, Mark S; et al. (December 11, 2014). "Clinical features and management of sepsis in the asplenic patient". UpToDate. Retrieved December 10, 2015.
- ↑ Anderson PA, Sleeper LA, Mahony L, et al. (2008). ""Contemporary outcomes after the Fontan procedure: A Pediatric Heart Network multicenter study."". Journal of the American College of Cardiology. 52 (2): 85–93. doi:10.1016/j.jacc.2008.01.074. PMC 4385517 . PMID 18598886.
- ↑ Shahrouki, Puja; Lee, Edward Wolfgang; Ruehm, Stefan (February 2022). "Polysplenia syndrome and sickle cell trait: extensive deep venous thrombosis from venous stasis and hypercoagulability". Clinical Imaging. 82: 127–131. doi:10.1016/j.clinimag.2021.11.017. ISSN 0899-7071. PMID 34813990. S2CID 244443675.
- ↑ Hashmi, Aijaz; Abu-Sulaiman, Riyadh; McCrindle, Brian W; Smallhorn, Jeffrey F; Williams, William G; Freedom, Robert M (1998-04-01). "Management and Outcomes of Right Atrial Isomerism: A 26-Year Experience". Journal of the American College of Cardiology. 31 (5): 1120–1126. doi: 10.1016/S0735-1097(98)00062-X . PMID 9562017.
- ↑ Mishra, Smita (2015-11-26). "Cardiac and Non-Cardiac Abnormalities in Heterotaxy Syndrome". The Indian Journal of Pediatrics. 82 (12): 1135–1146. doi:10.1007/s12098-015-1925-x. ISSN 0019-5456. PMID 26612104. S2CID 207388492.
- ↑ Lopez, Keila N.; Marengo, Lisa K.; Canfield, Mark A.; Belmont, John W.; Dickerson, Heather A. (2015-09-01). "Racial disparities in heterotaxy syndrome". Birth Defects Research Part A: Clinical and Molecular Teratology. 103 (11): 941–950. doi:10.1002/bdra.23416. ISSN 1542-0760. PMID 26333177.
- ↑ Kim, Soo-Jin; Kim, Woong-Han; Lim, Hong-Gook; Lee, Jae-Young (July 2008). "Outcome of 200 patients after an extracardiac Fontan procedure". The Journal of Thoracic and Cardiovascular Surgery. 136 (1): 108–116. doi:10.1016/j.jtcvs.2007.12.032. hdl: 10371/60103 . PMID 18603062.
- ↑ Lin, Angela E.; Krikov, Sergey; Riehle-Colarusso, Tiffany; Frías, Jaime L.; Belmont, John; Anderka, Marlene; Geva, Tal; Getz, Kelly D.; Botto, Lorenzo D. (2014-10-01). "Laterality defects in the national birth defects prevention study (1998–2007): Birth prevalence and descriptive epidemiology". American Journal of Medical Genetics Part A. 164 (10): 2581–2591. doi:10.1002/ajmg.a.36695. ISSN 1552-4833. PMC 4462240 . PMID 25099286.