Containment and control
| | This section needs expansion. You can help by adding to it. (February 2023) |
| 1997 Sarawak HFMD outbreak | |
|---|---|
| Disease | Enterovirus 71 |
| Index case | April 1997 |
| Confirmed cases | 600 |
Deaths | 28–31 |
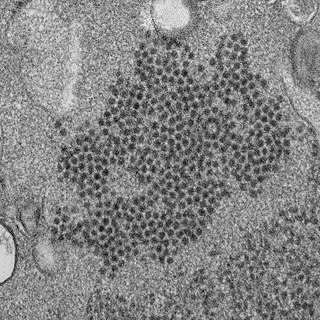
The 1997 Sarawak HFMD outbreak is a hand, foot, and mouth disease (HFMD) outbreak from April until June caused by the Enterovirus 71 (EV-71) affecting 600 children in the state of Sarawak in Malaysia. [1] [2] Sarawak is the first state in Malaysia that reported HFMD outbreak. An estimated 28 to 31 of the infected children died as a result. [3] [4] The affected children are aged between five months to six years. [4]
No data was available for HFMD or EV-71 in Malaysia before the 1997 outbreak. [4] In the midst of the outbreak in Sarawak, Coxsackie B virus (CV-B) was initially thought to be the causative agent based on the clinical presentation of myocarditis, but not detected among the deceased children. Instead, EV-71 was isolated from these fatal cases. After a few months, Enterovirus-71 was isolated from deceased children in Peninsular Malaysia that died from brainstem encephalomyelitis. [4]
Generally, HFMD disease symptoms can range from asymptomatic to symptoms associated with the upper respiratory tract, gastrointestinal tract, central nervous system, and cardiovascular system. Up to 71% of EV-71 infections are asymptomatic. [4]
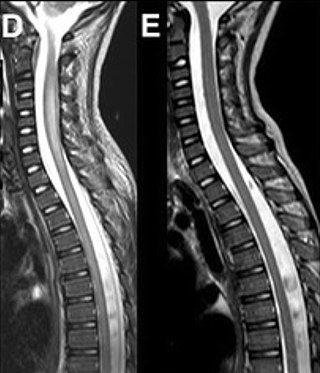
EV-71 infection can be divided into four stages. Stage 1 of EV-71 infection is uncomplicated and can manifest as HFMD or herpangina. Other types of viruses such as Coxsackievirus A4, A5, A10, B2, and B5 can also cause HFMD. Incubation period (period of time from exposure of the virus to the appearance of symptoms) ranges from three to seven days. An infected person can spread the disease several days before the symptoms appear and peak one week after the onset of the disease. Common symptoms at this stage are fever, sore throat, exanthem (especially maculopapular rash) at palms, feet, and buttocks. The disease can also affect the oral cavity, causing vesicles (small blisters) and ulcers on the tongue and soft palate. If only the oral cavity is affected, without the involvement of other body parts, it is known as herpangina. Most HFMD and herpangina are mild diseases and will resolve by themselves. [4] Stage 2 of the disease occurs a few days after stage I, and can be caused by EV-71 or echoviruses. Stage 2 is characterised by central nervous system involvement, causing meningoencephalitis, and polio-like syndrome such as poliomyelitis-like paralysis, and non-paralytic poliomyelitis (aseptic meningitis). EV-71 subgenotypes C1 and B5 are more likely to cause central nervous system infection when compared to subgenotype B4. Meningoencephalitis is the most common manifestation of the disease, while poliomyelitis-like paralysis is the least common. [4] Stage 3 of the disease signifies involvement of the heart and lungs. Stage 4 of the disease signifies long-term neurological consequences after the child recovered from the illness. [4]
Once infected with Cosackie A virus, it provides immunity against repeated infection with other serotypes of Cosackcie A viruses. However, Cosackie A virus infection does not provide immunity against EV-71 virus infection. Questions remain about whether an EV-71 virus infection provides immunity against other serotypes of EV-71 virus infection. [4]
Swabs done on skin vesicle, ulcer, oral, thorat, rectal, stool, and cerebrospinal fluid have shown EV-71 and Cosackie A16 was the most frequent isolated viruses isolated in Sarawak. [4]
In Sarawak, the most frequent symptoms of a child with central nervous system involvement are fever more than 38 degree Celsius for more than 3 days and lethargy. [4]
Through autopsies performed on the deceased children, their deaths are caused by several symptoms linked to the disease such as poor peripheral perfusion, tachycardia and cardiac failures with earlier developed symptoms such as shock, pallor, cold extremities, delayed capillary refill and weak peripheral pulses. [3]
Human is the only known reservoir for EV-71. The faecal-oral route is the main mode of transmission. Another mode of transmission is through respiratory droplets. EV-71 virus may continuously shed into faeces up to 42 days after the infection, longer than its shedding into the throat. [3] Children usually get infected in childcare facilities or get it from household contacts. Adults usually do not show any symptoms of HFMD, but may shed the virus and infect other children in the process. Enterovirus may persist in the environment for three days under room temperatures such as in sewage and water systems. Transmission through blood is rare. Although enteroviruses are generally transmitted to newborns during delivery, however, there is only one case reported for EV-71 transmission during delivery. [3]
| | This section needs expansion. You can help by adding to it. (February 2023) |
The majority of the HFMD infections are of stage I which do not require hospitalisation and can be treated symptomatically. Those with stage II disease is hospitalised and monitored. Immunoglobulin therapy is used in stage II to reduce the risk of death. The exact mechanism of immunoglobulin therapy in treating the disease is unknown, but it can reduce the level of inflammatory markers produced against the EV-71 virus in children with pulmonary oedema (accumulation of water within lung tissues and air spaces. A high level of inflammatory markers causes cytokine storm which is life-threatening instead of helping to fight against the infection. In those with stage III HFMD, intensive care support is required. Milrinone can be useful in increasing the cardiac output. In those with stage IV disease with limb weakness, limb atrophy and dysphagia, physical therapy is needed. Long-term respiratory support is needed for those with dysfunctioning thoracic diaphragm. [4]
EV-71 can infect the heart muscles, causing acute viral myocarditis that ultimately leads to acute congestive heart failure, cardiovascular collapse, and death. [4] [5] Dual infection with other enteroviruses or adenovirus does not increase the risk of neurological complications. [4]
| | This section needs expansion. You can help by adding to it. (February 2023) |
HFMD outbreaks in Sarawak continued in 3-yearly cycles in 2003, 2006, and 2008/2009 with deaths reported in each of the outbreak. EV-71 was seen during the years of the outbreak while Cosackie-A16 virus was seen during the years between the outbreaks. As of 2011, EV-71 type B4 and B5 were the most common variant that circulate in Sarawak. [4] HFMD cases usually increased between March and June during surveillance of the disease from 1998 to 2005. [4]
On 12 October 2006, statutory notification of HFMD is enforced. In 2007, Ministry of Health Malaysia released HFMD management guidelines. [4] Under this guideline, two or more HFMD cases reported in a childcare facility should be closed for 10 days from the last case detected and should be thoroughly disinfected. [4]

Poliomyelitis, commonly shortened to polio, is an infectious disease caused by the poliovirus. Approximately 75% of cases are asymptomatic; mild symptoms which can occur include sore throat and fever; in a proportion of cases more severe symptoms develop such as headache, neck stiffness, and paresthesia. These symptoms usually pass within one or two weeks. A less common symptom is permanent paralysis, and possible death in extreme cases. Years after recovery, post-polio syndrome may occur, with a slow development of muscle weakness similar to that which the person had during the initial infection.
Coxsackie A virus (CAV) is a cytolytic Coxsackievirus of the Picornaviridae family, an enterovirus.

Mumps is a viral disease caused by the mumps virus. Initial symptoms of mumps are non-specific and include fever, headache, malaise, muscle pain, and loss of appetite. These symptoms are usually followed by painful swelling of the parotid glands, called parotitis, which is the most common symptom of a mumps infection. Symptoms typically occur 16 to 18 days after exposure to the virus and resolve within two weeks. About one third of infections are asymptomatic.

Bornholm disease, also known as epidemic pleurodynia, is a condition characterized by myositis of the abdomen or chest caused by the Coxsackie B virus or other viruses. The myositis manifests as an intermittent stabbing pain in the musculature that is seen primarily in children and young adults.

Viral meningitis, also known as aseptic meningitis, is a type of meningitis due to a viral infection. It results in inflammation of the meninges. Symptoms commonly include headache, fever, sensitivity to light and neck stiffness.

Hand, foot, and mouth disease (HFMD) is a common infection caused by a group of enteroviruses. It typically begins with a fever and feeling generally unwell. This is followed a day or two later by flat discolored spots or bumps that may blister, on the hands, feet and mouth and occasionally buttocks and groin. Signs and symptoms normally appear 3–6 days after exposure to the virus. The rash generally resolves on its own in about a week. Fingernail and toenail loss may occur a few weeks later, but they will regrow with time.
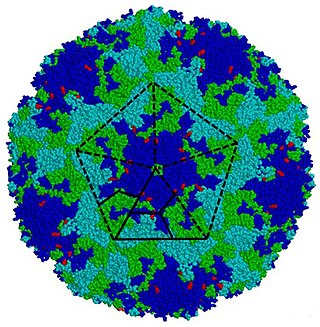
Coxsackie B4 virus are enteroviruses that belong to the Picornaviridae family. These viruses can be found worldwide. They are positive-sense, single-stranded, non-enveloped RNA viruses with icosahedral geometry. Coxsackieviruses have two groups, A and B, each associated with different diseases. Coxsackievirus group A is known for causing hand-foot-and-mouth diseases while Group B, which contains six serotypes, can cause a varying range of symptoms like gastrointestinal distress myocarditis. Coxsackievirus B4 has a cell tropism for natural killer cells and pancreatic islet cells. Infection can lead to beta cell apoptosis which increases the risk of insulitis.
Coxsackieviruses are a few related enteroviruses that belong to the Picornaviridae family of nonenveloped, linear, positive-sense single-stranded RNA viruses, as well as its genus Enterovirus, which also includes poliovirus and echovirus. Enteroviruses are among the most common and important human pathogens, and ordinarily its members are transmitted by the fecal–oral route. Coxsackieviruses share many characteristics with poliovirus. With control of poliovirus infections in much of the world, more attention has been focused on understanding the nonpolio enteroviruses such as coxsackievirus.
Coxsackie B is a group of six serotypes of coxsackievirus (CVB1-CVB6), a pathogenic enterovirus, that trigger illness ranging from gastrointestinal distress to full-fledged pericarditis and myocarditis.
Poliovirus, the causative agent of polio, is a serotype of the species Enterovirus C, in the family of Picornaviridae. There are three poliovirus serotypes: types 1, 2, and 3.
Enterovirus is a genus of positive-sense single-stranded RNA viruses associated with several human and mammalian diseases. Enteroviruses are named by their transmission-route through the intestine.

Aseptic meningitis is the inflammation of the meninges, a membrane covering the brain and spinal cord, in patients whose cerebral spinal fluid test result is negative with routine bacterial cultures. Aseptic meningitis is caused by viruses, mycobacteria, spirochetes, fungi, medications, and cancer malignancies. The testing for both meningitis and aseptic meningitis is mostly the same. A cerebrospinal fluid sample is taken by lumbar puncture and is tested for leukocyte levels to determine if there is an infection and goes on to further testing to see what the actual cause is. The symptoms are the same for both meningitis and aseptic meningitis but the severity of the symptoms and the treatment can depend on the certain cause.

Viral encephalitis is inflammation of the brain parenchyma, called encephalitis, by a virus. The different forms of viral encephalitis are called viral encephalitides. It is the most common type of encephalitis and often occurs with viral meningitis. Encephalitic viruses first cause infection and replicate outside of the central nervous system (CNS), most reaching the CNS through the circulatory system and a minority from nerve endings toward the CNS. Once in the brain, the virus and the host's inflammatory response disrupt neural function, leading to illness and complications, many of which frequently are neurological in nature, such as impaired motor skills and altered behavior.

Gingivostomatitis is a combination of gingivitis and stomatitis, or an inflammation of the oral mucosa and gingiva. Herpetic gingivostomatitis is often the initial presentation during the first ("primary") herpes simplex infection. It is of greater severity than herpes labialis which is often the subsequent presentations. Primary herpetic gingivostomatitis is the most common viral infection of the mouth.
Adenovirus infection is a contagious viral disease, caused by adenoviruses, commonly resulting in a respiratory tract infection. Typical symptoms range from those of a common cold, such as nasal congestion, coryza and cough, to difficulty breathing as in pneumonia. Other general symptoms include fever, fatigue, muscle aches, headache, abdominal pain and swollen neck glands. Onset is usually two to fourteen days after exposure to the virus. A mild eye infection may occur on its own, combined with a sore throat and fever, or as a more severe adenoviral keratoconjunctivitis with a painful red eye, intolerance to light and discharge. Very young children may just have an earache. Adenovirus infection can present as a gastroenteritis with vomiting, diarrhoea and abdominal pain, with or without respiratory symptoms. However, some people have no symptoms.

Enterovirus 71 (EV71), also known as Enterovirus A71 (EV-A71), is a virus of the genus Enterovirus in the Picornaviridae family, notable for its role in causing epidemics of severe neurological disease and hand, foot, and mouth disease in children. It was first isolated and characterized from cases of neurological disease in California in 1969. Enterovirus 71 infrequently causes polio-like syndrome permanent paralysis.
The central nervous system (CNS) controls most of the functions of the body and mind. It comprises the brain, spinal cord and the nerve fibers that branch off to all parts of the body. The CNS viral diseases are caused by viruses that attack the CNS. Existing and emerging viral CNS infections are major sources of human morbidity and mortality.
Enterovirus D68 (EV-D68) is a member of the Picornaviridae family, an enterovirus. First isolated in California in 1962 and once considered rare, it has been on a worldwide upswing in the 21st century. It is suspected of causing a polio-like disorder called acute flaccid myelitis (AFM).
Acute flaccid myelitis (AFM) is a serious condition of the spinal cord. Symptoms include rapid onset of arm or leg weakness and decreased reflexes. Difficulty moving the eyes, speaking, or swallowing may also occur. Occasionally, numbness or pain may be present. Complications can include trouble breathing.
Beginning in January 2018, an outbreak of hand, foot, and mouth disease (HFMD) occurred among children nationwide across Malaysia. Nearly 38,000 cases were recorded between January 1 and July 26, and by August 14 the total number of cases had risen to 51,000. Among the states and federal territories affected by the outbreak, Selangor recorded the highest cases with 11,349, Kuala Lumpur with 4,428 and Sarawak with 4,412 cases as reported in July 2018. At least two children in Sarawak and Penang died from complications caused by the virus.
In April 1997, in Sarawak, Malaysia, 600 cases of HFMD were admitted and over 30 children died.
