
The lymphatic system, or lymphoid system, is an organ system in vertebrates that is part of the immune system, and complementary to the circulatory system. It consists of a large network of lymphatic vessels, lymph nodes, lymphoid organs, lymphatic tissue and lymph. Lymph is a clear fluid carried by the lymphatic vessels back to the heart for re-circulation. The Latin word for lymph, lympha, refers to the deity of fresh water, "Lympha".
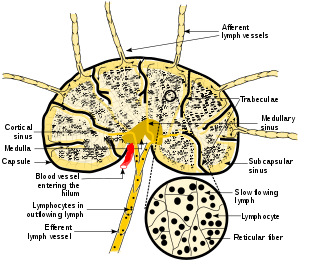
A lymph node, or lymph gland, is a kidney-shaped organ of the lymphatic system and the adaptive immune system. A large number of lymph nodes are linked throughout the body by the lymphatic vessels. They are major sites of lymphocytes that include B and T cells. Lymph nodes are important for the proper functioning of the immune system, acting as filters for foreign particles including cancer cells, but have no detoxification function.

Metastasis is a pathogenic agent's spread from an initial or primary site to a different or secondary site within the host's body; the term is typically used when referring to metastasis by a cancerous tumor. The newly pathological sites, then, are metastases (mets). It is generally distinguished from cancer invasion, which is the direct extension and penetration by cancer cells into neighboring tissues.

In human anatomy, the thoracic duct is the larger of the two lymph ducts of the lymphatic system. The thoracic duct usually begins from the upper aspect of the cisterna chyli, passing out of the abdomen through the aortic hiatus into first the posterior mediastinum and then the superior mediastinum, extending as high up as the root of the neck before descending to drain into the systemic (blood) circulation at the venous angle.
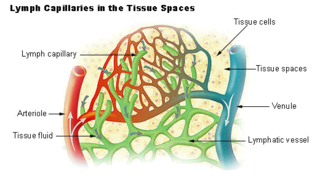
The lymphatic vessels are thin-walled vessels (tubes), structured like blood vessels, that carry lymph. As part of the lymphatic system, lymph vessels are complementary to the cardiovascular system. Lymph vessels are lined by endothelial cells, and have a thin layer of smooth muscle, and adventitia that binds the lymph vessels to the surrounding tissue. Lymph vessels are devoted to the propulsion of the lymph from the lymph capillaries, which are mainly concerned with the absorption of interstitial fluid from the tissues. Lymph capillaries are slightly bigger than their counterpart capillaries of the vascular system. Lymph vessels that carry lymph to a lymph node are called afferent lymph vessels, and those that carry it from a lymph node are called efferent lymph vessels, from where the lymph may travel to another lymph node, may be returned to a vein, or may travel to a larger lymph duct. Lymph ducts drain the lymph into one of the subclavian veins and thus return it to general circulation.

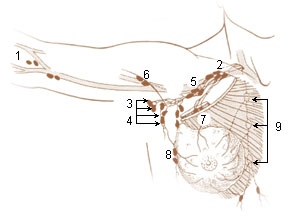
The axilla is the area on the human body directly under the shoulder joint. It includes the axillary space, an anatomical space within the shoulder girdle between the arm and the thoracic cage, bounded superiorly by the imaginary plane between the superior borders of the first rib, clavicle and scapula, medially by the serratus anterior muscle and thoracolumbar fascia, anteriorly by the pectoral muscles and posteriorly by the subscapularis, teres major and latissimus dorsi muscle.

Lymphadenopathy or adenopathy is a disease of the lymph nodes, in which they are abnormal in size or consistency. Lymphadenopathy of an inflammatory type is lymphadenitis, producing swollen or enlarged lymph nodes. In clinical practice, the distinction between lymphadenopathy and lymphadenitis is rarely made and the words are usually treated as synonymous. Inflammation of the lymphatic vessels is known as lymphangitis. Infectious lymphadenitis affecting lymph nodes in the neck is often called scrofula.
Courvoisier's principle states that a painless palpably enlarged gallbladder accompanied with mild jaundice is unlikely to be caused by gallstones. Usually, the term is used to describe the physical examination finding of the right-upper quadrant of the abdomen. This sign implicates possible malignancy of the gallbladder or pancreas and the swelling is unlikely due to gallstones.

Inguinal lymph nodes are lymph nodes in the groin. They are situated in the femoral triangle of the inguinal region. They are subdivided into two groups: the superficial inguinal lymph nodes and deep inguinal lymph nodes.

A chylothorax is an abnormal accumulation of chyle, a type of lipid-rich lymph, in the pleural space surrounding the lung. The lymphatics of the digestive system normally returns lipids absorbed from the small bowel via the thoracic duct, which ascends behind the esophagus to drain into the left brachiocephalic vein. If normal thoracic duct drainage is disrupted, either due to obstruction or rupture, chyle can leak and accumulate within the negative-pressured pleural space. In people on a normal diet, this fluid collection can sometimes be identified by its turbid, milky white appearance, since chyle contains emulsified triglycerides.
The uterine sarcomas form a group of malignant tumors that arises from the smooth muscle or connective tissue of the uterus. They can be difficult to detect, as symptoms are common to other uterine conditions and no specific screening test has been developed. This presents an issue for treatment, as the cancer spreads quickly.
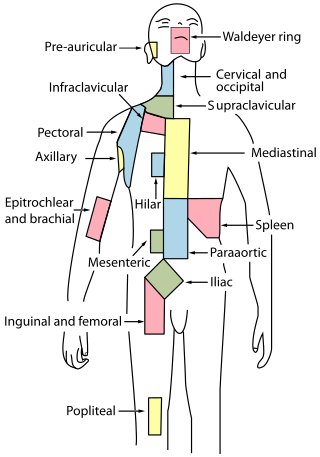
Cervical lymph nodes are lymph nodes found in the neck. Of the 800 lymph nodes in the human body, 300 are in the neck. Cervical lymph nodes are subject to a number of different pathological conditions including tumours, infection and inflammation.

The axillary lymph nodes or armpit lymph nodes are lymph nodes in the human armpit. Between 20 and 49 in number, they drain lymph vessels from the lateral quadrants of the breast, the superficial lymph vessels from thin walls of the chest and the abdomen above the level of the navel, and the vessels from the upper limb. They are divided in several groups according to their location in the armpit. These lymph nodes are clinically significant in breast cancer, and metastases from the breast to the axillary lymph nodes are considered in the staging of the disease.

The bronchomediastinal lymph trunks are essential components of the human lymphatic system, tasked with draining lymph from the tracheobronchial, internal mammary, and anterior mediastinal lymph nodes.
The parasternal lymph nodes are placed at the anterior ends of the intercostal spaces, by the side of the internal thoracic artery.

Medullary breast carcinoma is a rare type of breast cancer that is characterized as a relatively circumscribed tumor with pushing, rather than infiltrating, margins. It is histologically characterized as poorly differentiated cells with abundant cytoplasm and pleomorphic high grade vesicular nuclei. It involves lymphocytic infiltration in and around the tumor and can appear to be brown in appearance with necrosis and hemorrhage. Prognosis is measured through staging but can often be treated successfully and has a better prognosis than other infiltrating breast carcinomas.

Cervical lymphadenopathy refers to lymphadenopathy of the cervical lymph nodes. The term lymphadenopathy strictly speaking refers to disease of the lymph nodes, though it is often used to describe the enlargement of the lymph nodes. Similarly, the term lymphadenitis refers to inflammation of a lymph node, but often it is used as a synonym of lymphadenopathy.
Lymph node metastasis is the spread (metastasis) of cancer cells into a lymph node.

Lymphovascular invasion is the invasion of a cancer to the blood vessels and/or lymphatics.



