| Eardrum | |
|---|---|
 | |
 Right eardrum as seen through a speculum | |
| Details | |
| Identifiers | |
| Latin | membrana tympanica; myringa |
| MeSH | D014432 |
| TA98 | A15.3.01.052 |
| TA2 | 6870 |
| FMA | 9595 |
| Anatomical terminology | |
 |
| This article is one of a series documenting the anatomy of the |
| Human ear |
|---|
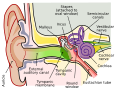
In the anatomy of humans and various other tetrapods, the eardrum, also called the tympanic membrane or myringa, is a thin, cone-shaped membrane that separates the external ear from the middle ear. Its function is to transmit changes in pressure of sound from the air to the ossicles inside the middle ear, and thence to the oval window in the fluid-filled cochlea. The ear thereby converts and amplifies vibration in the air to vibration in cochlear fluid. [1] The malleus bone bridges the gap between the eardrum and the other ossicles. [2]
Contents
- Structure
- Orientation and relations
- Regions
- Umbo
- Nerve supply
- Clinical significance
- Examination
- Rupture
- Surgical puncture for treatment of middle ear infections
- Society and culture
- See also
- Additional images
- References
- External links
Rupture or perforation of the eardrum can lead to conductive hearing loss. Collapse or retraction of the eardrum can cause conductive hearing loss or cholesteatoma.