GnRH was discovered in 1971, and GnRH analogues were introduced for medical use in the 1980s.[6][7] Their nonproprietary names usually end in -relin. The most well-known and widely used GnRH analogues are leuprorelin (brand name Lupron) and triptorelin (brand name Decapeptyl). GnRH analogues are available as generic medications. Despite this, they continue to be very expensive.
Medical uses
GnRH agonists are used medically to manage hormone-related conditions such as uterine fibroids and endometriosis, precocious puberty, and hormone-sensitive cancers like prostate and breast cancer, as well as in fertility treatments to control the timing of ovulation. GnRH agonists that have been marketed and are available for medical use include buserelin, gonadorelin, goserelin, histrelin, leuprorelin, nafarelin, and triptorelin. GnRH agonists that are used mostly or exclusively in veterinary medicine include deslorelin and fertirelin. GnRH agonists can be administered by injection, by implant, or intranasally as a nasal spray. Injectables have been formulated for daily, monthly, and quarterly use, and implants are available that can last from one month to a year. With the exception of gonadorelin, which is used as a progonadotropin, all approved GnRH agonists are used as antigonadotropins. The clinically used desensitizing GnRH agonists are available in the following pharmaceutical formulations:[8][9][10][11]
Treatment of cancers that are hormonally sensitive and where a hypogonadal state decreases the chances of a recurrence. Thus they are commonly employed in the medical management of prostate cancer and have been used in patients with breast cancer.[citation needed]
Puberty
GnRH agonists are used in puberty treatment primarily to manage precocious puberty (early onset of puberty) by suppressing the release of sex hormones, to slow pubertal progression until an appropriate age.[citation needed] They are also used in gender-affirming care to delay puberty in transgender and non-binary youth, providing time to explore gender identity before irreversible physical changes occur.[citation needed]
Women of reproductive age who undergo cytotoxic chemotherapy have been pretreated with GnRH agonists to reduce the risk of oocyte loss during such therapy and preserve ovarian function. Further studies are necessary to prove that this approach is useful.[15]
Summary of available forms
GnRH agonists marketed for clinical or veterinary use
Common side effects of the GnRH agonists and antagonists include symptoms of hypogonadism such as hot flashes, gynecomastia, fatigue, weight gain, fluid retention, erectile dysfunction and decreased libido. Long term therapy can result in metabolic abnormalities, weight gain, worsening of diabetes and osteoporosis. Rare, but potentially serious adverse events include transient worsening of prostate cancer due to surge in testosterone with initial injection of GnRH agonists and pituitary apoplexy in patients with pituitary adenoma. Single instances of clinically apparent liver injury have been reported with some GnRH agonists (histrelin, goserelin), but the reports were not very convincing. There is no evidence to indicate that there is cross sensitivity to liver injury among the various GnRH analogues despite their similarity in structure.[16] There is also a report that GnRH agonists used in the treatment of advanced prostate cancer may increase the risk of heart problems by 30%.[17]
Pharmacology
GnRH agonists act as agonists of the GnRH receptor, the biological target of gonadotropin-releasing hormone (GnRH). These drugs can be both peptides and small-molecules. They are modeled after the hypothalamicneurohormone GnRH, which interacts with the GnRH receptor to elicit its biologic response, the release of the pituitaryhormonesfollicle-stimulating hormone (FSH) and luteinizing hormone (LH). However, after the initial "flare" response, continued stimulation with GnRH agonists desensitizes the pituitary gland (by causing GnRH receptor downregulation) to GnRH. Pituitary desensitization reduces the secretion of LH and FSH and thus induces a state of hypogonadotropic hypogonadal anovulation, sometimes referred to as "pseudomenopause" or "medical oophorectomy".[1] GnRH agonists are able to completely shutdown gonadal testosterone production and thereby suppress circulating testosterone levels by 95% or into the castrate/female range in men.[5]
Agonists do not quickly dissociate from the GnRH receptor. As a result, initially there is an increase in FSH and LH secretion (so-called "flare effect"). Levels of LH may increase by up to 10-fold,[18][19] while levels of testosterone generally increase to 140 to 200% of baseline values.[20] However, after continuous administration, a profound hypogonadal effect (i.e. decrease in FSH and LH) is achieved through receptor downregulation by internalization of receptors.[18] Generally this induced and reversible hypogonadism is the therapeutic goal. During the flare, peak levels of testosterone occur after 2 to 4days, baseline testosterone levels are returned to by 7 to 8days, and castrate levels of testosterone are achieved by two to fourweeks.[20][18] A 7 day study of infertile women found that restoration of normal gonadotropin secretion takes 5 to 8 days after cessation of exogenous GnRH agonists.[21]
Testosterone levels during the first month of androgen deprivation therapy in men with prostate cancer treated with subcutaneous injections of a GnRH antagonist (degarelix) or agonist (leuprorelin). Doses were 240 then 80 mg/month and 7.5 mg/month, respectively.[28]
Testosterone levels in the long-term androgen deprivation therapy of men with prostate cancer by different GnRH agonists administered at 3 month intervals (goserelin, triptorelin and leuprorelin). Dotted line is the threshold for the castrate range.[29]
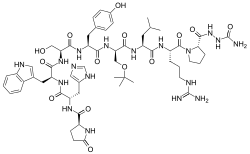
GnRH agonists are synthetically modeled after the natural GnRH decapeptide with specific modifications, usually double and single substitutions and typically in position 6 (amino acid substitution), 9 (alkylation) and 10 (deletion). These substitutions inhibit rapid degradation. Agonists with two substitutions include: leuprorelin, buserelin, histrelin, goserelin, and deslorelin. The agents nafarelin and triptorelin are agonists with single substitutions at position 6.[citation needed]
↑LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Gonadotropin Releasing Hormone (GnRH) Analogues. [Updated 2018 Mar 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547863/
12Krakowsky Y, Morgentaler A (July 2017). "Risk of Testosterone Flare in the Era of the Saturation Model: One More Historical Myth". Eur Urol Focus. 5 (1): 81–89. doi:10.1016/j.euf.2017.06.008. PMID28753828. S2CID10011200. Initial administration of LHRH agonists reliably causes a transient rise in serum T, with peak T values observed at 2–4 d followed by a reduction to baseline values by 7–8 d, and achievement of castrate levels by 2–4 wk [10]. Most studies demonstrate an increase in peak serum T concentrations by 40–100% above baseline during T flare.
↑Cedrin-Durnerin I, Bidart JM, Robert P, Wolf JP, Uzan M, Hugues JN (May 2000). "Consequences on gonadotrophin secretion of an early discontinuation of gonadotrophin-releasing hormone agonist administration in short-term protocol for in-vitro fertilization". Human Reproduction. 15 (5): 1009–14. doi:10.1093/humrep/15.5.1009. PMID10783343.
12Vis AN, van der Sluis TM, Al-Itejawi HH, van Moorselaar RJ, Meuleman EJ (January 2015). "Risk of disease flare with LHRH agonist therapy in men with prostate cancer: myth or fact?". Urol. Oncol. 33 (1): 7–15. doi:10.1016/j.urolonc.2014.04.016. PMID25159013.
↑Shimizu TS, Shibata Y, Jinbo H, Satoh J, Yamanaka H (1995). "Estramustine phosphate for preventing flare-up in luteinizing hormone-releasing hormone analogue depot therapy". Eur. Urol. 27 (3): 192–5. doi:10.1159/000475159. PMID7541359.
↑Sugiono M, Winkler MH, Okeke AA, Benney M, Gillatt DA (2005). "Bicalutamide vs cyproterone acetate in preventing flare with LHRH analogue therapy for prostate cancer--a pilot study". Prostate Cancer Prostatic Dis. 8 (1): 91–4. doi:10.1038/sj.pcan.4500784. PMID15711607. S2CID9151853.
↑Klotz L, Boccon-Gibod L, Shore ND, Andreou C, Persson BE, Cantor P, Jensen JK, Olesen TK, Schröder FH (December 2008). "The efficacy and safety of degarelix: a 12-month, comparative, randomized, open-label, parallel-group phase III study in patients with prostate cancer". BJU Int. 102 (11): 1531–8. doi:10.1111/j.1464-410X.2008.08183.x. PMID19035858.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.
 Testosterone levels during the first month of androgen deprivation therapy in men with prostate cancer treated with subcutaneous injections of a GnRH antagonist (degarelix) or agonist (leuprorelin). Doses were 240 then 80 mg/month and 7.5 mg/month, respectively. [28]
Testosterone levels during the first month of androgen deprivation therapy in men with prostate cancer treated with subcutaneous injections of a GnRH antagonist (degarelix) or agonist (leuprorelin). Doses were 240 then 80 mg/month and 7.5 mg/month, respectively. [28] Testosterone levels in the long-term androgen deprivation therapy of men with prostate cancer by different GnRH agonists administered at 3 month intervals (goserelin, triptorelin and leuprorelin). Dotted line is the threshold for the castrate range. [29]
Testosterone levels in the long-term androgen deprivation therapy of men with prostate cancer by different GnRH agonists administered at 3 month intervals (goserelin, triptorelin and leuprorelin). Dotted line is the threshold for the castrate range. [29]