Tobacco smoking is the practice of burning tobacco and ingesting the resulting smoke. The smoke may be inhaled, as is done with cigarettes, or simply released from the mouth, as is generally done with pipes and cigars. The practice is believed to have begun as early as 5000–3000 BC in Mesoamerica and South America. Tobacco was introduced to Eurasia in the late 17th century by European colonists, where it followed common trade routes. The practice encountered criticism from its first import into the Western world onwards but embedded itself in certain strata of a number of societies before becoming widespread upon the introduction of automated cigarette-rolling apparatus.

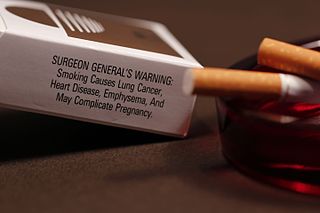
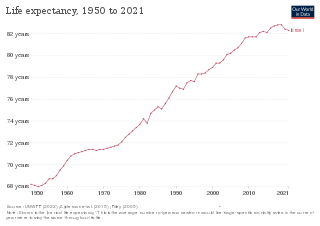
Tobacco products, especially when smoked or used orally, have serious negative effects on human health. Smoking and smokeless tobacco use are the single greatest causes of preventable death globally. Half of tobacco users die from complications related to such use. Current smokers are estimated to die an average of 10 years earlier than non-smokers. The World Health Organization estimates that, in total, about 8 million people die from tobacco-related causes, including 1.3 million non-smokers due to secondhand smoke. It is further estimated to have caused 100 million deaths in the 20th century.

Prevalence of tobacco use is reported by the World Health Organization (WHO), which focuses on cigarette smoking due to reported data limitations. Smoking has therefore been studied more extensively than any other form of consumption.
Tobacco harm reduction (THR) is a public health strategy to lower the health risks to individuals and wider society associated with using tobacco products. It is an example of the concept of harm reduction, a strategy for dealing with the use of drugs. Tobacco smoking is widely acknowledged as a leading cause of illness and death, and reducing smoking is vital to public health.

Smoking is a practice in which a substance is combusted and the resulting smoke is typically inhaled to be tasted and absorbed into the bloodstream of a person. Most commonly, the substance used is the dried leaves of the tobacco plant, which have been rolled with a small rectangle of paper into an elongated cylinder called a cigarette. Other forms of smoking include the use of a smoking pipe or a bong.

Flavored tobacco products — tobacco products with added flavorings — include types of cigarettes, cigarillos and cigars, hookahs and hookah tobacco, various types of smokeless tobacco, and more recently electronic cigarettes. Flavored tobacco products are especially popular with youth and have therefore become targets of regulation in several countries.
Health in Israel is generally considered good.
Tobacco control is a field of international public health science, policy and practice dedicated to addressing tobacco use and thereby reducing the morbidity and mortality it causes. Since most cigarettes and cigars and hookahs contain/use tobacco, tobacco control also concerns these. E-cigarettes do not contain tobacco itself, but (often) do contain nicotine. Tobacco control is a priority area for the World Health Organization (WHO), through the Framework Convention on Tobacco Control. References to a tobacco control movement may have either positive or negative connotations, depending upon the commentator.
Tobacco has a long cultural, economic, and social impact on the United States. Tobacco cultivation in Jamestown, Virginia, in 1610 led to the expansion of British colonialism in the Southern United States. As the demand for Tobacco grew in Europe, further colonization in British America and Tobacco production saw a parallel increase. Tobacco use became normalized in American society and was heavily consumed before and after American independence.
Smoking in China is prevalent, as the People's Republic of China is the world's largest consumer and producer of tobacco. As of 2022, there are around 300 million Chinese smokers, and 2.4 trillion cigarettes are sold there every year, 46% of the world total.

Smokingamong youth and adolescents is an issue that affects countries worldwide. While the extent to which smoking is viewed as a negative health behavior may vary across different nations, it remains an issue regardless of how it is perceived by different societies. The United States has taken numerous measures, ranging from changes in national policy surrounding youth cigarette access to changes in media campaigns, in attempts to eliminate the use of tobacco products among teenagers. Approximately 90% of smokers begin smoking prior to the age of 18.

The majority of lifelong smokers begin smoking habits before the age of 24, which makes the college years a critical time for tobacco companies to convince college students to pick up the habit of cigarette smoking. Cigarette smoking in college is seen as a social activity by those who partake in it, and more than half of the students that are users do not consider themselves smokers. This may be because most college students plan to quit smoking by the time that they graduate.

Cigarette smoking for weight loss is a weight control method whereby one consumes tobacco, often in the form of cigarettes, to decrease one's appetite. The practice dates to early knowledge of nicotine as an appetite suppressant.

Smoking in Syria is steadily increasing in popularity amongst the Syrian population, mainly in the forms of cigarettes or narghiles. In Syria, the General Organization of Tobacco manages the growth and exportation of tobacco products. Syrians collectively spend about $600 million per year on tobacco consumption. As of 2010, 20% of women and 60% of men smoke and 98% of the overall population is affected by passive smoking. Narghiles and cigarettes are the two main forms of tobacco consumption. Despite the assumption that smoking, specifically the narghile, is embedded in Syrian culture, this phenomenon has only recently become widespread. Health officials are currently working on smoking cessation programs and policies, to remove this idea that smoking in Syria is an essential part of the culture, to educate regarding health effects, and to prevent citizens from smoking in public places.

The use of tobacco products in Egypt is widespread. It is estimated that approximately twenty percent of the population uses tobacco products daily. Cigarettes are the most common form of tobacco consumption in Egypt, with an estimated twenty billion cigarettes smoked annually in the country. After cigarettes, shisha water-pipes are the most common form of tobacco consumption.

Smoking in Albania is prevalent as about 40% of Albanians smoke regularly. In Europe, only Turkey has a higher smoking rate than Albania. Albanians annually spend more than €300 million on tobacco products. Zog I of Albania was reported to smoke 200 cigarettes a day. Albania adopted tough anti-smoking laws in 2007, but they are not strictly enforced. Smoking prevalence is increasing, especially among females ages 13 to 15. The smoking rate for teens between the ages of 13 and 15 is currently 15%.

Tobacco smoking is popular in North Korea and culturally acceptable among men, but not for women. As of 2019, some 43.6% of men are reported to smoke daily, whilst in contrast only 4.5% of women smoke daily, with most of these being older women from rural areas. Smoking is a leading cause of death in North Korea, and as of 2021 mortality figures indicate that 14.2% of North Koreans die due to smoking-related causes, which is the 6th highest rate after China, Greenland, Kiribati, Denmark and Micronesia. There are tobacco control programs in North Korea, and although smoking was not prohibited in all public spaces, the smoking rates have declined since their peak in the 2000s.

Tobacco policy in Armenia is the attempt by the Armenian authorities to regulate smoking in Armenia. Tobacco laws and regulations are controlled by the Ministry of Health of Armenia. Armenian men tend to be the most common tobacco users, as 42.5% of men over the age of 15 smoke.
Smoking in Australia is restricted in enclosed public places, workplaces, in areas of public transport and near underage events, except new laws in New South Wales that ban smoking within ten metres of children's play spaces.
Smoking in Croatia is legally permitted, with certain restrictions. Smoking is banned in all enclosed public spaces, with the exception of psychiatric wards and designated smoking rooms. All direct or indirect advertisement of tobacco or smoking is banned as well. All tobacco product packaging must, by law, display health warnings.

