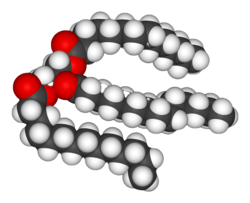
Idealized representation of a molecule of a typical triglyceride, the main type of fat. Note the three fatty acid chains attached to the central glycerol portion of the molecule.Composition of fats from various foods, as percentage of their total fat
The term often refers specifically to triglycerides (triple esters of glycerol), that are the main components of vegetable oils and of fatty tissue in animals;[2] or, even more narrowly, to triglycerides that are solid or semisolid at room temperature, thus excluding oils. The term may also be used more broadly as a synonym of lipid—any substance of biological relevance, composed of carbon, hydrogen, or oxygen, that is insoluble in water but soluble in non-polar solvents.[1] In this sense, besides the triglycerides, the term would include several other types of compounds like mono- and diglycerides, phospholipids (such as lecithin), sterols (such as cholesterol), waxes (such as beeswax),[1] and free fatty acids, which are usually present in human diet in smaller amounts.[2]
In humans and many animals, fats serve both as energy sources and as stores for energy in excess of what the body needs immediately. Each gram of fat when burned or metabolized releases about nine food calories(37 kJ = 8.8 kcal).[5]
Fats are also sources of essential fatty acids, an important dietary requirement. Vitamins A, D, E, and K are fat-soluble, meaning they can only be digested, absorbed, and transported in conjunction with fats.
Fats play a vital role in maintaining healthy skin and hair, insulating body organs against shock, maintaining body temperature, and promoting healthy cell function. Fat also serves as a useful buffer against a host of diseases. When a particular substance, whether chemical or biotic, reaches unsafe levels in the bloodstream, the body can effectively dilute—or at least maintain equilibrium of—the offending substances by storing it in new fat tissue.[6] This helps to protect vital organs, until such time as the offending substances can be metabolized or removed from the body by such means as excretion, urination, accidental or intentional bloodletting, sebum excretion, and hair growth.
Adipose tissue
The obese mouse (left) has large stores of adipose tissue. For comparison, a mouse with a normal amount of adipose tissue is also shown (right).
In animals, adipose tissue (fatty tissue) is the body's means of storing metabolic energy over extended periods of time. Adipocytes (fat cells) store fat derived from the diet and from liver metabolism. Under energy stress these cells may degrade their stored fat to supply fatty acids and also glycerol to the circulation. These metabolic activities are regulated by several hormones (e.g., insulin, glucagon and epinephrine). Adipose tissue also secretes the hormone leptin.[7]
Production and processing
A variety of chemical and physical techniques are used for the production and processing of fats, both industrially and in cottage or home settings. They include:
The pancreatic lipase acts at the ester bond, hydrolyzing the bond and "releasing" the fatty acid. In triglyceride form, lipids cannot be absorbed by the duodenum. Fatty acids, monoglycerides (one glycerol, one fatty acid), and some diglycerides are absorbed by the duodenum, once the triglycerides have been broken down.
In the intestine, following the secretion of lipases and bile, triglycerides are split into monoacylglycerol and free fatty acids in a process called lipolysis. They are subsequently moved to absorptive enterocyte cells lining the intestines. The triglycerides are rebuilt in the enterocytes from their fragments and packaged together with cholesterol and proteins to form chylomicrons. These are excreted from the cells and collected by the lymph system and transported to the large vessels near the heart before being mixed into the blood. Various tissues can capture the chylomicrons, releasing the triglycerides to be used as a source of energy. Liver cells can synthesize and store triglycerides. When the body requires fatty acids as an energy source, the hormone glucagon signals the breakdown of the triglycerides by hormone-sensitive lipase to release free fatty acids. As the brain cannot utilize fatty acids as an energy source (unless converted to a ketone),[8] the glycerol component of triglycerides can be converted into glucose, via gluconeogenesis by conversion into dihydroxyacetone phosphate and then into glyceraldehyde 3-phosphate, for brain fuel when it is broken down. Fat cells may also be broken down for that reason if the brain's needs ever outweigh the body's.
Triglycerides cannot pass through cell membranes freely. Special enzymes on the walls of blood vessels called lipoprotein lipases must break down triglycerides into free fatty acids and glycerol. Fatty acids can then be taken up by cells via fatty acid transport proteins (FATPs).
Triglycerides, as major components of very-low-density lipoprotein (VLDL) and chylomicrons, play an important role in metabolism as energy sources and transporters of dietary fat. They contain more than twice as much energy (approximately 9kcal/g or 38kJ/g) as carbohydrates (approximately 4kcal/g or 17kJ/g).[9]
Nutritional and health aspects
The most common type of fat, in human diet and most living beings, is a triglyceride, an ester of the triple alcoholglycerolH(–CHOH–) 3H and three fatty acids. The molecule of a triglyceride can be described as resulting from a condensation reaction (specifically, esterification) between each of glycerol's –OH groups and the HO– part of the carboxyl group HO(O=)C− of each fatty acid, forming an ester bridge−O−(O=)C− with elimination of a water molecule H 2O.
Other less common types of fats include diglycerides and monoglycerides, where the esterification is limited to two or just one of glycerol's –OH groups. Other alcohols, such as cetyl alcohol (predominant in spermaceti), may replace glycerol. In the phospholipids, one of the fatty acids is replaced by phosphoric acid or a monoester thereof. The benefits and risks of various amounts and types of dietary fats have been the object of much study, and are still highly controversial topics.[10][11][12][13]
Different foods contain different amounts of fat with different proportions of saturated and unsaturated fatty acids. Some animal products, like beef and dairy products made with whole or reduced fat milk like yogurt, ice cream, cheese and butter have mostly saturated fatty acids (and some have significant contents of dietary cholesterol). Other animal products, like pork, poultry, eggs, and seafood have mostly unsaturated fats. Industrialized baked goods may use fats with high unsaturated fat contents as well, especially those containing partially hydrogenated oils, and processed foods that are deep-fried in hydrogenated oil are high in saturated fat content.[44][45][46]
Many scientific studies have found that replacing saturated fats with cis unsaturated fats in the diet reduces risk of cardiovascular diseases (CVDs),[49]diabetes, or death.[50] These studies prompted many medical organizations and public health departments, including the World Health Organization (WHO),[51][52] to officially issue that advice. Some countries with such recommendations include:
A 2004 review concluded that "no lower safe limit of specific saturated fatty acid intakes has been identified" and recommended that the influence of varying saturated fatty acid intakes against a background of different individual lifestyles and genetic backgrounds should be the focus in future studies.[69]
This advice is often oversimplified by labeling the two kinds of fats as bad fats and good fats, respectively. However, since the fats and oils in most natural and traditionally processed foods contain both unsaturated and saturated fatty acids,[70] the complete exclusion of saturated fat is unrealistic and possibly unwise. For instance, some foods rich in saturated fat, such as coconut and palm oil, are an important source of cheap dietary calories for a large fraction of the population in developing countries.[71]
Concerns were also expressed at a 2010 conference of the American Dietetic Association that a blanket recommendation to avoid saturated fats could drive people to also reduce the amount of polyunsaturated fats, which may have health benefits, and/or replace fats by refined carbohydrates — which carry a high risk of obesity and heart disease.[72]
For these reasons, the U.S. Food and Drug Administration, for example, recommends to consume less than 10% (7% for high-risk groups) of calories from saturated fat, with 15-30% of total calories from all fat.[73][71] A general 7% limit was recommended also by the American Heart Association (AHA) in 2006.[74][75]
The WHO/FAO report also recommended replacing fats so as to reduce the content of myristic and palmitic acids, specifically.[71]
The so-called Mediterranean diet, prevalent in many countries in the Mediterranean Sea area, includes more total fat than the diet of Northern European countries, but most of it is in the form of unsaturated fatty acids (specifically, monounsaturated and omega-3) from olive oil and fish, vegetables, and certain meats like lamb, while consumption of saturated fat is minimal in comparison. A 2017 review found evidence that a Mediterranean-style diet could reduce the risk of cardiovascular diseases, overall cancer incidence, neurodegenerative diseases, diabetes, and mortality rate.[76] A 2018 review showed that a Mediterranean-like diet may improve overall health status, such as reduced risk of non-communicable diseases. It also may reduce the social and economic costs of diet-related illnesses.[77]
A small number of contemporary reviews have challenged this negative view of saturated fats. For example, an evaluation of evidence from 1966 to 1973 of the observed health impact of replacing dietary saturated fat with linoleic acid found that it increased rates of death from all causes, coronary heart disease, and cardiovascular disease.[78] These studies have been disputed by many scientists,[79] and the consensus in the medical community is that saturated fat and cardiovascular disease are closely related.[80][81][82] Still, these discordant studies fueled debate over the merits of substituting polyunsaturated fats for saturated fats.[83]
The effect of saturated fat on cardiovascular disease has been extensively studied.[49] The general consensus is that there is evidence of moderate-quality of a strong, consistent, and graded relationship between saturated fat intake, blood cholesterol levels, and the incidence of cardiovascular disease.[50][49] The relationships are accepted as causal,[84][85] including by many government and medical organizations.[71][86][87][50][88][89][90][91]
A 2017 review by the AHA estimated that replacement of saturated fat with polyunsaturated fat in the American diet could reduce the risk of cardiovascular diseases by 30%.[50]
The consumption of saturated fat is generally considered a risk factor for dyslipidemia—abnormal blood lipid levels, including high total cholesterol, high levels of triglycerides, high levels of low-density lipoprotein (LDL, "bad" cholesterol) or low levels of high-density lipoprotein (HDL, "good" cholesterol). These parameters in turn are believed to be risk indicators for some types of cardiovascular disease.[92][93][94][95][96][88][97][98][99] These effects were observed in children too.[100]
Several meta-analyses (reviews and consolidations of multiple previously published experimental studies) have confirmed a significant relationship between saturated fat and high serum cholesterol levels,[50][101] which in turn have been claimed to have a causal relation with increased risk of cardiovascular disease (the so-called lipid hypothesis).[102][103] However, high cholesterol may be caused by many factors. Other indicators, such as high LDL/HDL ratio, have proved to be more predictive.[103] In a study of myocardial infarction in 52 countries, the ApoB/ApoA1 (related to LDL and HDL, respectively) ratio was the strongest predictor of CVD among all risk factors.[104] There are other pathways involving obesity, triglyceride levels, insulin sensitivity, endothelial function, and thrombogenicity, among others, that play a role in CVD, although it seems, in the absence of an adverse blood lipid profile, the other known risk factors have only a weak atherogenic effect.[105] Different saturated fatty acids have differing effects on various lipid levels.[106]
Cancer
The evidence for a relation between saturated fat intake and cancer is significantly weaker, and there does not seem to be a clear medical consensus about it.
Several reviews of case–control studies have found that saturated fat intake is associated with increased breast cancer risk.[107][108][109]
Another review found limited evidence for a positive relationship between consuming animal fat and incidence of colorectal cancer.[110]
Other meta-analyses found evidence for increased risk of ovarian cancer by high consumption of saturated fat.[111]
Some studies have indicated that serum myristic acid[112][113] and palmitic acid[113] and dietary myristic[114] and palmitic[114] saturated fatty acids and serum palmitic combined with alpha-tocopherol supplementation[112] are associated with increased risk of prostate cancer in a dose-dependent manner. These associations may, however, reflect differences in intake or metabolism of these fatty acids between the precancer cases and controls, rather than being an actual cause.[113]
Bones
Various animal studies have indicated that the intake of saturated fat has a negative effect on the mineral density of bones. One study suggested that men may be particularly vulnerable.[115]
Disposition and overall health
Studies have shown that substituting monounsaturated fatty acids for saturated ones is associated with increased daily physical activity and resting energy expenditure. More physical activity, less anger, and less irritability were associated with a higher-oleic acid diet than one of a palmitic acid diet.[116]
Amounts of fat types in selected foods
Monounsaturated vs. polyunsaturated fat
Schematic diagram of a triglyceride with a saturated fatty acid (top), a monounsaturated one (middle) and a polyunsaturated one (bottom)
MUFAs (especially oleic acid) have been found to lower the incidence of insulin resistance; PUFAs (especially large amounts of arachidonic acid) and SFAs (such as arachidic acid) increased it. These ratios can be indexed in the phospholipids of human skeletal muscle and in other tissues as well. The relationship between dietary fats and insulin resistance is presumed secondary to the relationship between insulin resistance and inflammation, which is partially modulated by dietary fat ratios (omega−3/6/9), with both omega–3 and –9 thought to be anti-inflammatory and omega–6 pro-inflammatory (as well as by numerous other dietary components, particularly polyphenols and exercise, with both of these anti-inflammatory). Although both pro- and anti-inflammatory types of fat are biologically necessary, fat dietary ratios in most U.S. diets are skewed towards omega–6, with subsequent disinhibition of inflammation and potentiation of insulin resistance.[70] This is contrary to the suggestion that polyunsaturated fats are shown to be protective against insulin resistance.[citation needed]
The large-scale KANWU study found that increasing MUFA and decreasing SFA intake could improve insulin sensitivity, but only when the overall fat intake of the diet was low.[127] However, some MUFAs may promote insulin resistance (like the SFAs), whereas PUFAs may protect against it.[128][129][clarification needed]
Cancer
Levels of oleic acid along with other MUFAs in red blood cell membranes were positively associated with breast cancer risk. The saturation index (SI) of the same membranes was inversely associated with breast cancer risk. MUFAs and low SI in erythrocyte membranes are predictors of postmenopausal breast cancer. Both of these variables depend on the activity of the enzyme delta-9 desaturase (Δ9-d).[130]
Results from observational clinical trials on PUFA intake and cancer have been inconsistent and vary by numerous factors of cancer incidence, including gender and genetic risk.[131] Some studies have shown associations between higher intakes and/or blood levels of omega-3 PUFAs and a decreased risk of certain cancers, including breast and colorectal cancer, while other studies found no associations with cancer risk.[131][132]
Pregnancy disorders
Polyunsaturated fat supplementation was found to have no effect on the incidence of pregnancy-related disorders, such as hypertension or preeclampsia, but may increase the length of gestation slightly and decreased the incidence of early premature births.[123]
Expert panels in the United States and Europe recommend that pregnant and lactating women consume higher amounts of polyunsaturated fats than the general population to enhance the DHA status of the fetus and newborn.[123]
In nature, unsaturated fatty acids generally have double bonds in cis configuration (with the adjacent C–C bonds on the same side) as opposed to trans.[133] Nevertheless, trans fatty acids (TFAs) occur in small amounts in meat and milk of ruminants (such as cattle and sheep),[134][135] typically 2–5% of total fat.[136] Natural TFAs, which include conjugated linoleic acid (CLA) and vaccenic acid, originate in the rumen of these animals. CLA has two double bonds, one in the cis configuration and one in trans, which makes it simultaneously a cis- and a trans-fatty acid.[137]
The trans fat content in various natural and traditionally processed foods is shown in the table below.
The processing of fats by hydrogenation can convert some unsaturated fats into trans fats. The presence of trans fats in various processed foods has received much attention.
Margarine is a common product that can contain trans fats.Cover of the original Crisco cookbook, 1912. Crisco was made by hydrogenating cottonseed oil. The formula was revised in the 2000s and now has only a small amount of trans fat.
The ω−3 fatty acids have received substantial attention. Among omega-3 fatty acids, neither long-chain nor short-chain forms were consistently associated with breast cancer risk. High levels of docosahexaenoic acid (DHA), however, the most abundant omega-3 polyunsaturated fatty acid in erythrocyte (red blood cell) membranes, were associated with a reduced risk of breast cancer.[130] The DHA obtained through the consumption of polyunsaturated fatty acids is positively associated with cognitive and behavioral performance.[139] In addition, DHA is vital for the grey matter structure of the human brain, as well as retinal stimulation and neurotransmission.[123]
Interesterification
Some studies have investigated the health effects of interesterified (IE) fats, by comparing diets with IE and non-IE fats with the same overall fatty acid composition.[140][141]
Several experimental studies in humans found no statistical difference on fasting blood lipids between a diet with large amounts of IE fat, having 25-40% C16:0 or C18:0 on the 2-position, and a similar diet with non-IE fat, having only 3-9% C16:0 or C18:0 on the 2-position.[142][143][144] A negative result was obtained also in a study that compared the effects on blood cholesterol levels of an IE fat product mimicking cocoa butter and the real non-IE product.[145][146][147][148][149][150][151] Another study found tentative evidence that interesterified fat may lower cardiovascular disease risk.[140]
A 2007 study funded by the Malaysian Palm Oil Board[152] claimed that replacing natural palm oil by other interesterified or partially hydrogenated fats caused adverse health effects, such as higher LDL/HDL ratio and plasma glucose levels. However, these effects could be attributed to the higher percentage of saturated acids in the IE and partially hydrogenated fats, rather than to the IE process itself.[153][154]
Unsaturated fats undergo auto-oxidation, which involves replacement of a C-H bond with C-OH unit. The process requires oxygen (air) and is accelerated by the presence of traces of metals, which serve as catalysts. Doubly unsaturated fatty acids are particularly prone to this reaction. Vegetable oils resist this process to a small degree because they contain antioxidants, such as tocopherol. Fats and oils often are treated with chelating agents such as citric acid to remove the metal catalysts.
In the human body, high levels of triglycerides in the bloodstream have been linked to atherosclerosis, heart disease[155] and stroke.[9] However, the relative negative impact of raised levels of triglycerides compared to that of LDL:HDL ratios is as yet unknown. The risk can be partly accounted for by a strong inverse relationship between triglyceride level and HDL-cholesterol level. But the risk is also due to high triglyceride levels increasing the quantity of small, dense LDL particles.[156]
The decision to treat hypertriglyceridemia with medication depends on the levels and on the presence of other risk factors for cardiovascular disease. Very high levels that would increase the risk of pancreatitis is treated with a drug from the fibrate class. Niacin and omega-3 fatty acids as well as drugs from the statin class may be used in conjunction, with statins being the main drug treatment for moderate hypertriglyceridemia where reduction of cardiovascular risk is required.[167][161] Medications are recommended in those with high levels of triglycerides that are not corrected with lifestyle modifications, with fibrates being recommended first.[161][168][169]Epanova (omega-3-carboxylic acids) is another prescription drug used to treat very high levels of blood triglycerides.[170]
12Drummond, K. E.; Brefere, L. M. (2014). Nutrition for Foodservice and Culinary Professionals (8thed.). John Wiley & Sons. ISBN978-0-470-05242-6.
↑Rebecca J. Donatelle (2005): Health, the Basics, 6th edition. Pearson Education, San Francisco; ISBN978-0-13-120687-8
↑Hu FB, Manson JE, Willett WC (2001). "Types of dietary fat and risk of coronary heart disease: A critical review". Journal of the American College of Nutrition. 20 (1): 5–19. doi:10.1080/07315724.2001.10719008.
↑Bray GA, Paeratakul S, Popkin BM (2004). "Dietary fat and obesity: a review of animal, clinical and epidemiological studies". Physiology & Behavior. 83 (4): 549–555. doi:10.1016/j.physbeh.2004.08.039. PMID15621059.
↑Mozaffarian D, Katan MB, Ascherio A, Stampfer MJ, Willett WC (2006). "Trans fatty acids and cardiovascular disease". New England Journal of Medicine. 354 (15): 1601–1613. doi:10.1056/NEJMra054035. PMID16611951.
123"FoodData Central". United States Department of Agriculture. April 1, 2019. All values in this table are from this database unless otherwise cited or when italicized as the simple arithmetic sum of other component columns.
↑"Brazil nut oil, fat composition, 100 g". US National Nutrient Database, Release 28, United States Department of Agriculture. May 2016. Retrieved September 6, 2017.
1234Katragadda, Harinageswara Rao; Fullana, Andrés; Sidhu, Sukh; Carbonell-Barrachina, Ángel A. (May 2010). "Emissions of volatile aldehydes from heated cooking oils". Food Chemistry. 120 (1): 59–65. doi:10.1016/j.foodchem.2009.09.070.
↑"Canola oil, fat composition, 100 g". US National Nutrient Database, Release 28, United States Department of Agriculture. May 2016. Retrieved September 6, 2017.
↑"Coconut oil, fat composition, 100 g". US National Nutrient Database, Release 28, United States Department of Agriculture. May 2016. Retrieved September 6, 2017.
↑"Palm oil, fat composition, 100 g". US National Nutrient Database, Release 28, United States Department of Agriculture. May 2016. Retrieved September 6, 2017.
↑Zelman K (2011). "The Great Fat Debate: A Closer Look at the Controversy—Questioning the Validity of Age-Old Dietary Guidance". Journal of the American Dietetic Association. 111 (5): 655–658. doi:10.1016/j.jada.2011.03.026. PMID21515106.
↑Dinu M, Pagliai G, Casini A, Sofi F (January 2018). "Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials". European Journal of Clinical Nutrition. 72 (1): 30–43. doi:10.1038/ejcn.2017.58. hdl:2158/1081996. PMID28488692. S2CID7702206.
↑Labarthe D (2011). "Chapter 17 What Causes Cardiovascular Diseases?". Epidemiology and prevention of cardiovascular disease: a global challenge (2nded.). Jones and Bartlett Publishers. ISBN978-0-7637-4689-6.
↑Kris-Etherton PM, Innis S (September 2007). "Position of the American Dietetic Association and Dietitians of Canada: Dietary Fatty Acids". Journal of the American Dietetic Association. 107 (9): 1599–1611 [1603]. doi:10.1016/j.jada.2007.07.024. PMID17936958.
↑"Cholesterol". Irish Heart Foundation. Retrieved February 28, 2011.
↑U.S. Department of Agriculture and U.S. Department of Health and Human Services (December 2010). Dietary Guidelines for Americans, 2010(PDF) (7thed.). Washington, DC: U.S. Government Printing Office.
↑Cannon C, O'Gara P (2007). Critical Pathways in Cardiovascular Medicine (2nded.). Lippincott Williams & Wilkins. p.243.
↑Catapano AL, Reiner Z, De Backer G, Graham I, Taskinen MR, Wiklund O, etal. (July 2011). "ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS)". Atherosclerosis. 217 Suppl 1 (14): S1-44. doi:10.1016/j.atherosclerosis.2011.06.012. hdl:10138/307445. PMID21723445.
↑"Monounsaturated Fat". American Heart Association. Archived from the original on March 7, 2018. Retrieved April 19, 2018.
↑Sanchez-Bayle M, Gonzalez-Requejo A, Pelaez MJ, Morales MT, Asensio-Anton J, Anton-Pacheco E (February 2008). "A cross-sectional study of dietary habits and lipid profiles. The Rivas-Vaciamadrid study". European Journal of Pediatrics. 167 (2): 149–54. doi:10.1007/s00431-007-0439-6. PMID17333272. S2CID8798248.
12Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R (December 2007). "Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths". Lancet. 370 (9602): 1829–39. Bibcode:2007Lanc..370.1829.. doi:10.1016/S0140-6736(07)61778-4. PMID18061058. S2CID54293528.
↑Labarthe D (2011). "Chapter 11 Adverse Blood Lipid Profile". Epidemiology and prevention of cardiovascular disease: a global challenge (2ed.). Jones and Bartlett Publishers. p.290. ISBN978-0-7637-4689-6.
↑Labarthe D (2011). "Chapter 11 Adverse Blood Lipid Profile". Epidemiology and prevention of cardiovascular disease: a global challenge (2nded.). Jones and Bartlett Publishers. p.277. ISBN978-0-7637-4689-6.
↑Thijssen MA, Mensink RP (2005). "Fatty acids and atherosclerotic risk". Atherosclerosis: Diet and Drugs. Handbook of Experimental Pharmacology. Vol.170. Springer. pp.165–194. doi:10.1007/3-540-27661-0_5. ISBN978-3-540-22569-0. PMID16596799.
↑Huncharek M, Kupelnick B (2001). "Dietary fat intake and risk of epithelial ovarian cancer: a meta-analysis of 6,689 subjects from 8 observational studies". Nutrition and Cancer. 40 (2): 87–91. doi:10.1207/S15327914NC402_2. PMID11962260. S2CID24890525.
↑Aizpurua-Olaizola O, Ormazabal M, Vallejo A, Olivares M, Navarro P, Etxebarria N, Usobiaga A (January 2015). "Optimization of supercritical fluid consecutive extractions of fatty acids and polyphenols from Vitis vinifera grape wastes". Journal of Food Science. 80 (1): E101-7. doi:10.1111/1750-3841.12715. PMID25471637.
12345"Essential Fatty Acids". Micronutrient Information Center, Oregon State University, Corvallis, OR. May 2014. Retrieved May 24, 2017.
↑Fukuchi S, Hamaguchi K, Seike M, Himeno K, Sakata T, Yoshimatsu H (June 2004). "Role of fatty acid composition in the development of metabolic disorders in sucrose-induced obese rats". Experimental Biology and Medicine. 229 (6): 486–93. doi:10.1177/153537020422900606. PMID15169967. S2CID20966659.
↑Tarrago-Trani MT, Phillips KM, Lemar LE, Holden JM (June 2006). "New and existing oils and fats used in products with reduced trans-fatty acid content". Journal of the American Dietetic Association. 106 (6): 867–80. doi:10.1016/j.jada.2006.03.010. PMID16720128.
↑van de Rest O, Geleijnse JM, Kok FJ, van Staveren WA, Dullemeijer C, Olderikkert MG, Beekman AT, de Groot CP (August 2008). "Effect of fish oil on cognitive performance in older subjects: a randomized, controlled trial". Neurology. 71 (6): 430–8. doi:10.1212/01.wnl.0000324268.45138.86. PMID18678826. S2CID45576671.
↑Zampelas A, Williams CM, Morgan LM, etal. (1994), "The effect of triacylglycerol fatty acids positional distribution on postprandial plasma metabolite and hormone responses in normal adult men.", Br J Nutr, vol.71, no.3, pp.401–410, doi:10.1079/bjn19940147, PMID8172869
↑Berry SE, Woodward R, Yeoh C, Miller GJ, Sanders TA (2007), "Effect of interesterification of palmitic-acid rich tryacylglycerol on postprandial lipid and factor VII response", Lipids, 42 (4): 315–323, doi:10.1007/s11745-007-3024-x, PMID17406926, S2CID3986807
↑Christophe AB, De Greyt WF, Delanghe JR, Huyghebaert AD (2000), "Substituting enzymically interesterified butter for native butter has no effect on lipemia or lipoproteinemia in man", Annals of Nutrition and Metabolism, 44 (2): 61–67, doi:10.1159/000012822, PMID10970994, S2CID22276158
↑Gill JM, Herd SL, Tsetsonis NV, Hardman AE (February 2002). "Are the reductions in triacylglycerol and insulin levels after exercise related?". Clinical Science. 102 (2): 223–231. doi:10.1042/cs20010204. PMID11834142.
↑European Association for Cardiovascular Prevention & Rehabilitation; Reiner, Zeljko; Catapano, Alberico L.; De Backer, Guy; Graham, Ian; Taskinen, Marja-Riitta; Wiklund, Olov; Agewall, Stefan; Alegria, Eduardo; Chapman, M. John; Durrington, Paul; Erdine, Serap; Halcox, Julian; Hobbs, Richard; Kjekshus, John (July 2011). "ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS)". European Heart Journal. 32 (14): 1769–1818. doi:10.1093/eurheartj/ehr158. ISSN1522-9645. PMID21712404.
↑Davidson MH, Cannon CP, Armani AM (January 28, 2008). "Pharmacological Therapy for Cardiovascular Disease". In Davidson MH, Toth PP, Maki KC (eds.). Therapeutic Lipidology. Contemporary Cardiology. Totowa, New Jersey: Humana Press, Inc. pp.141–142. ISBN978-1-58829-551-4.
↑Abourbih S, Filion KB, Joseph L, Schiffrin EL, Rinfret S, Poirier P, etal. (October 2009). "Effect of fibrates on lipid profiles and cardiovascular outcomes: a systematic review". The American Journal of Medicine. 122 (10): 962.e1–962.e8. doi:10.1016/j.amjmed.2009.03.030. PMID19698935.
↑Jun M, Foote C, Lv J, Neal B, Patel A, Nicholls SJ, etal. (May 2010). "Effects of fibrates on cardiovascular outcomes: a systematic review and meta-analysis". Lancet. 375 (9729): 1875–1884. doi:10.1016/S0140-6736(10)60656-3. PMID20462635. S2CID15570639.
↑Blair HA, Dhillon S (October 2014). "Omega-3 carboxylic acids (Epanova): a review of its use in patients with severe hypertriglyceridemia". American Journal of Cardiovascular Drugs. 14 (5): 393–400. doi:10.1007/s40256-014-0090-3. PMID25234378. S2CID23706094.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.