
Human teeth function to mechanically break down items of food by cutting and crushing them in preparation for swallowing and digesting. As such, they are considered part of the human digestive system. Humans have four types of teeth: incisors, canines, premolars, and molars, which each have a specific function. The incisors cut the food, the canines tear the food and the molars and premolars crush the food. The roots of teeth are embedded in the maxilla or the mandible and are covered by gums. Teeth are made of multiple tissues of varying density and hardness.

Bruxism is excessive teeth grinding or jaw clenching. It is an oral parafunctional activity; i.e., it is unrelated to normal function such as eating or talking. Bruxism is a common behavior; reports of prevalence range from 8% to 31% in the general population. Several symptoms are commonly associated with bruxism, including aching jaw muscles, headaches, hypersensitive teeth, tooth wear, and damage to dental restorations. Symptoms may be minimal, without patient awareness of the condition. If nothing is done, after a while many teeth start wearing down until the whole tooth is gone.

Tooth enamel is one of the four major tissues that make up the tooth in humans and many other animals, including some species of fish. It makes up the normally visible part of the tooth, covering the crown. The other major tissues are dentin, cementum, and dental pulp. It is a very hard, white to off-white, highly mineralised substance that acts as a barrier to protect the tooth but can become susceptible to degradation, especially by acids from food and drink. Calcium hardens the tooth enamel. In rare circumstances enamel fails to form, leaving the underlying dentin exposed on the surface.

A mouthguard is a protective device for the mouth that covers the teeth and gums to prevent and reduce injury to the teeth, arches, lips and gums. An effective mouthguard is like a crash helmet for teeth and jaws. It also prevents the jaws coming together fully, thereby reducing the risk of jaw joint injuries and concussion. A mouthguard is most often used to prevent injury in contact sports, as a treatment for bruxism or TMD, or as part of certain dental procedures, such as tooth bleaching or sleep apnea treatment. Depending on the application, it may also be called a mouth protector, mouth piece, gumshield, gumguard, nightguard, occlusal splint, bite splint, or bite plane. The dentists who specialise in sports dentistry fabricate mouthguards.

In dentistry, a crown or a dental cap is a type of dental restoration that completely caps or encircles a tooth or dental implant. A crown may be needed when a large dental cavity threatens the health of a tooth. A crown is typically bonded to the tooth by dental cement. They can be made from various materials, which are usually fabricated using indirect methods. Crowns are used to improve the strength or appearance of teeth and to halt deterioration. While beneficial to dental health, the procedure and materials can be costly.

Abrasion is the non-carious, mechanical wear of tooth from interaction with objects other than tooth-tooth contact. It most commonly affects the premolars and canines, usually along the cervical margins. Based on clinical surveys, studies have shown that abrasion is the most common but not the sole aetiological factor for development of non-carious cervical lesions (NCCL) and is most frequently caused by incorrect toothbrushing technique.

Acid erosion is a type of tooth wear. It is defined as the irreversible loss of tooth structure due to chemical dissolution by acids not of bacterial origin. Dental erosion is the most common chronic condition of children ages 5–17, although it is only relatively recently that it has been recognised as a dental health problem. There is generally widespread ignorance of the damaging effects of acid erosion; this is particularly the case with erosion due to consumption of fruit juices because they tend to be considered as healthy. Acid erosion begins initially in the enamel, causing it to become thin, and can progress into dentin, giving the tooth a dull yellow appearance and leading to dentin hypersensitivity.
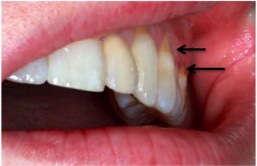
Abfraction is a theoretical concept explaining a loss of tooth structure not caused by tooth decay. It is suggested that these lesions are caused by forces placed on the teeth during biting, eating, chewing and grinding; the enamel, especially at the cementoenamel junction (CEJ), undergoes large amounts of stress, causing micro fractures and tooth tissue loss. Abfraction appears to be a modern condition, with examples of non-carious cervical lesions in the archaeological record typically caused by other factors.

Dentinogenesis imperfecta (DI) is a genetic disorder of tooth development. It is inherited in an autosomal dominant pattern, as a result of mutations on chromosome 4q21, in the dentine sialophosphoprotein gene (DSPP). It is one of the most frequently occurring autosomal dominant features in humans. Dentinogenesis imperfecta affects an estimated 1 in 6,000-8,000 people.
Dens evaginatus is a rare odontogenic developmental anomaly that is found in teeth where the outer surface appears to form an extra bump or cusp.
Talon cusp is a rare dental anomaly resulting in an extra cusp or cusp-like projection on an anterior tooth, located on the inside surface of the affected tooth. Sometimes it can also be found on the facial surface of the anterior tooth.
Dental anatomy is a field of anatomy dedicated to the study of human tooth structures. The development, appearance, and classification of teeth fall within its purview. Tooth formation begins before birth, and the teeth's eventual morphology is dictated during this time. Dental anatomy is also a taxonomical science: it is concerned with the naming of teeth and the structures of which they are made, this information serving a practical purpose in dental treatment.
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.
Dental pertains to the teeth, including dentistry. Topics related to the dentistry, the human mouth and teeth include:

Cracked tooth syndrome (CTS) is where a tooth has incompletely cracked but no part of the tooth has yet broken off. Sometimes it is described as a greenstick fracture. The symptoms are very variable, making it a notoriously difficult condition to diagnose.
The Dahl effect or Dahl concept is used in dentistry where a localized appliance or localized restoration is used to increase the available interocclusal space for restorations.

Tooth wear refers to loss of tooth substance by means other than dental caries. Tooth wear is a very common condition that occurs in approximately 97% of the population. This is a normal physiological process occurring throughout life; but with increasing lifespan of individuals and increasing retention of teeth for life, the incidence of non-carious tooth surface loss has also shown a rise. Tooth wear varies substantially between people and groups, with extreme attrition and enamel fractures common in archaeological samples, and erosion more common today.

Tooth mobility is the horizontal or vertical displacement of a tooth beyond its normal physiological boundaries around the gingival area, i.e. the medical term for a loose tooth.

Non-carious cervical lesions (NCCLs) are a group of lesions that are characterised by a loss of hard dental tissue at the cementoenamel junction (CEJ) region at the neck of the tooth, without the action of microorganisms or inflammatory processes. These lesions vary in shape from regular depressions that look like a dome or a cup, to deep wedge-shaped defects with the apex pointing inwards. NCCLs can occur either above or below the level of the gum, at any of the surfaces of the teeth.
Occlusion according to The Glossary of Prosthodontic Terms Ninth Edition is defined as 'the static relationship between the incising or masticating surfaces of the maxillary or mandibular teeth or tooth analogues'.

