Related Research Articles

The salivary glands in many vertebrates including mammals are exocrine glands that produce saliva through a system of ducts. Humans have three paired major salivary glands, as well as hundreds of minor salivary glands. Salivary glands can be classified as serous, mucous, or seromucous (mixed).

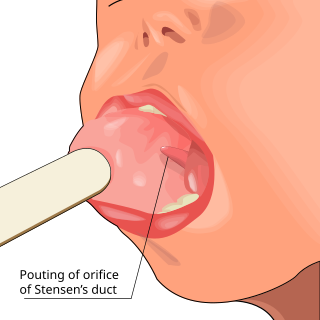
The parotid gland is a major salivary gland in many animals. In humans, the two parotid glands are present on either side of the mouth and in front of both ears. They are the largest of the salivary glands. Each parotid is wrapped around the mandibular ramus, and secretes serous saliva through the parotid duct into the mouth, to facilitate mastication and swallowing and to begin the digestion of starches. There are also two other types of salivary glands; they are submandibular and sublingual glands. Sometimes accessory parotid glands are found close to the main parotid glands.
The paired submandibular glands are major salivary glands located beneath the floor of the mouth. In adult humans, they each weigh about 15 grams and contribute some 60–67% of unstimulated saliva secretion; on stimulation their contribution decreases in proportion as parotid gland secretion rises to 50%. The average length of the normal adult human submandibular salivary gland is approximately 27 mm, while the average width is approximately 14.3 mm.
Parotitis is an inflammation of one or both parotid glands, the major salivary glands located on either side of the face, in humans. The parotid gland is the salivary gland most commonly affected by inflammation.
The oral mucosa is the mucous membrane lining the inside of the mouth. It comprises stratified squamous epithelium, termed "oral epithelium", and an underlying connective tissue termed lamina propria. The oral cavity has sometimes been described as a mirror that reflects the health of the individual. Changes indicative of disease are seen as alterations in the oral mucosa lining the mouth, which can reveal systemic conditions, such as diabetes or vitamin deficiency, or the local effects of chronic tobacco or alcohol use. The oral mucosa tends to heal faster and with less scar formation compared to the skin. The underlying mechanism remains unknown, but research suggests that extracellular vesicles might be involved.

Warthin's tumor, also known as papillary cystadenoma lymphomatosum, is a benign cystic tumor of the salivary glands containing abundant lymphocytes and germinal centers. It is named for pathologist Aldred Scott Warthin, who described two cases in 1929.

Pleomorphic adenoma is a common benign salivary gland neoplasm characterised by neoplastic proliferation of epithelial (ductal) cells along with myoepithelial components, having a malignant potentiality. It is the most common type of salivary gland tumor and the most common tumor of the parotid gland. It derives its name from the architectural Pleomorphism seen by light microscopy. It is also known as "Mixed tumor, salivary gland type", which refers to its dual origin from epithelial and myoepithelial elements as opposed to its pleomorphic appearance.
An oral medicine or stomatology doctor/dentist has received additional specialized training and experience in the diagnosis and management of oral mucosal abnormalities including oral cancer, salivary gland disorders, temporomandibular disorders and facial pain, taste and smell disorders; and recognition of the oral manifestations of systemic and infectious diseases. It lies at the interface between medicine and dentistry. An oral medicine doctor is trained to diagnose and manage patients with disorders of the orofacial region.

Mucoepidermoid carcinoma (MEC) is the most common type of minor salivary gland malignancy in adults. Mucoepidermoid carcinoma can also be found in other organs, such as bronchi, lacrimal sac, and thyroid gland.

Sialadenitis (sialoadenitis) is inflammation of salivary glands, usually the major ones, the most common being the parotid gland, followed by submandibular and sublingual glands. It should not be confused with sialadenosis (sialosis) which is a non-inflammatory enlargement of the major salivary glands.

Sialolithiasis is a crystallopathy where a calcified mass or sialolith forms within a salivary gland, usually in the duct of the submandibular gland. Less commonly the parotid gland or rarely the sublingual gland or a minor salivary gland may develop salivary stones.

Acinic cell carcinoma is a malignant tumor representing 2% of all salivary tumors. 90% of the time found in the parotid gland, 10% intraorally on buccal mucosa or palate. The disease presents as a slow growing mass, associated with pain or tenderness in 50% of the cases. Often appears pseudoencapsulated.

The Stafne defect is a depression of the mandible, most commonly located on the lingual surface. The Stafne defect is thought to be a normal anatomical variant, as the depression is created by ectopic salivary gland tissue associated with the submandibular gland and does not represent a pathologic lesion as such. This cavity is commonly observed on panoramic radiograph.

Salivary gland tumours, also known as mucous gland adenomas or neoplasms, are tumours that form in the tissues of salivary glands. The salivary glands are classified as major or minor. The major salivary glands consist of the parotid, submandibular, and sublingual glands. The minor salivary glands consist of 800 to 1000 small mucus-secreting glands located throughout the lining of the oral cavity. Patients with these types of tumours may be asymptomatic.
Sialoendoscopy is a minimally invasive technique that allows for salivary gland surgery for the safe and effective treatment of obstructive salivary gland disorders and other conditions of the salivary glands. During sialoendoscopy a small endoscope is placed into the salivary glands through the salivary ducts that empty into the mouth. The procedure is not exclusively diagnostic, but is interventional; thus, it can be used for the extraction of salivary stones, salivary duct lavage, dilatation of stenotic segments, or instillation of various medications such as corticosteroids or antibiotics. Thus, sialoendoscopy is an efficient yet simple mode of treatment for major salivary gland obstructions, strictures and sialoliths. Depending on the obstruction, sialoendoscopy can be conducted under local anesthesia in an outpatient office or in the operating room under general anesthesia.

IgG4-related disease (IgG4-RD), formerly known as IgG4-related systemic disease, is a chronic inflammatory condition characterized by tissue infiltration with lymphocytes and IgG4-secreting plasma cells, various degrees of fibrosis (scarring) and a usually prompt response to oral steroids. In approximately 51–70% of people with this disease, serum IgG4 concentrations are elevated during an acute phase.
A sialoblastoma is a low-grade salivary gland neoplasm that recapitulates primitive salivary gland anlage. It has previously been referred to as congenital basal cell adenoma, embryoma, or basaloid adenocarcinoma. It is an extremely rare tumor, with less than 100 cases reported worldwide.

Salivary gland diseases (SGDs) are multiple and varied in cause. There are three paired major salivary glands in humans: the parotid glands, the submandibular glands, and the sublingual glands. There are also about 800–1,000 minor salivary glands in the mucosa of the mouth. The parotid glands are in front of the ears, one on side, and secrete mostly serous saliva, via the parotid ducts, into the mouth, usually opening roughly opposite the second upper molars. The submandibular gland is medial to the angle of the mandible, and it drains its mixture of serous and mucous saliva via the submandibular duct into the mouth, usually opening in a punctum in the floor of mouth. The sublingual gland is below the tongue, on the floor of the mouth; it drains its mostly mucous saliva into the mouth via about 8–20 ducts, which open along the plica sublingualis, a fold of tissue under the tongue.
Sialodochitis, is inflammation of the duct system of a salivary gland. This is compared to sialadenitis, which is inflammation of the gland parenchyma.

Sclerosing polycystic adenosis is a rare salivary gland tumor first described in 1996 by Dr. Brion Smith. The major salivary glands, specifically the parotid gland and the submandibular gland, are affected most commonly. Patients usually come to clinical attention with a mass or swelling in their salivary glands in the 5th decade of life, with females affected much more commonly than males. Nearly all of the cases reported so far have a benign behavior, although there is a single case that has had an associated malignant transformation.
References
- ↑ John H. Stone; Arezou Khosroshahi; Vikram Deshpande; et al. (October 2012). "Recommendations for the nomenclature of IgG4-related disease and its individual organ system manifestations". Arthritis & Rheumatism. 64 (10): 3061–3067. doi:10.1002/art.34593. PMC 5963880 . PMID 22736240.
- ↑ Küttner, H (1896). "Ueber entzündliche Tumoren der submaxillar-speicheldrüse". Beiträge zur Klinischen Chirurgie. 15: 815–828. hdl:2027/uc1.b3731679.
- ↑ Kiverniti, E; Singh A; Clarke P (2008). "Küttner's tumour: an unusual cause of salivary gland enlargement". Hippokratia. 12 (1): 56–58. PMC 2532958 . PMID 18923750.
- ↑ Blanco, Mario; Mesko T; Cura M; Cabello-Inchausti B (2003). "Chronic sclerosing sialadenitis (Kuttner's tumor): unusual presentation with bilateral involvement of major and minor salivary glands". Annals of Diagnostic Pathology. 7 (1): 25–30. doi:10.1053/adpa.2003.50004. PMID 12616471.
- ↑ Beriat, GK; Akmansu SH; Kocatürk S; Ataoğlu O (2010). "Chronic Sclerosing Sialadenitis (Küttner's tumour) of the Parotid Gland". Malaysian Journal of Medical Sciences. 17 (4): 57–61. PMC 3216182 . PMID 22135562.
- 1 2 de Vicente, JC; López-Arranz E; García J; López-Arranz JS (2003). "Chronic sclerosing sialadenitis of the parotid gland". Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 96 (1): 77–80. doi:10.1016/s1079-2104(03)00096-9. PMID 12847448.
- ↑ Speight, PM; Barrett AW (2002). "Salivary gland tumours". Oral Diseases. 8 (5): 229–240. doi: 10.1034/j.1601-0825.2002.02870.x . PMID 12363107.
- ↑ National Cancer Institute (NCI/NIH) (20 July 2012). "General Information About Salivary Gland Cancer". cancer.gov. Archived from the original on 27 April 2015. Retrieved 15 November 2013.
- ↑ Chan ACL; Chan JKC; Abbondanzo SL (2005). "Chapter 5. Tumours of the Salivary Glands" (PDF). In Leon Barnes; John W. Eveson; Peter Reichart; David Sidransky (eds.). World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. Lyon, France: WHO/IARC Press. p. 278. ISBN 92-83-22417-5. Archived from the original (PDF) on 1 April 2017. Retrieved 15 November 2013.
- ↑ Epivatianos, A; Harrison JD; Dimitriou T (2006). "Ultrastructural and histochemical observations on microcalculi in chronic submandibular sialadenitis". Journal of Oral Pathology and Medicine. 16 (10): 514–517. doi:10.1111/j.1600-0714.1987.tb00683.x. PMID 3127566.
- ↑ Chan, JKC (1998). "Kuttner tumor (chronic sclerosing sialadenitis) of the submandibular gland: an underrecognized entity". Advances in Anatomic Pathology. 5 (4): 239–51. doi:10.1097/00125480-199807000-00004. PMID 9859756. S2CID 33288884.
- ↑ Ikeda, M; Ikui A; Tanaka M; Omori H; Tomita H (1994). "Immunohistopathological investigation on unspecific chronic sclerosing sialadenitis of the submandibular gland (Kuttner tumor)". Auris Nasus Larynx. 21 (2): 103–110. doi:10.1016/s0385-8146(12)80028-9. PMID 7993223.
- ↑ Tiemann, M; Teymoortash A; Schrader C; Werner JA; Parwaresch R; Seifert G; Klöppel G (2002). "Chronic sclerosing sialadenitis of the submandibular gland is mainly due to a T lymphocyte immune reaction". Modern Pathology. 15 (8): 845–852. doi: 10.1097/01.MP.0000022280.72359.04 . PMID 12181270.
- ↑ Tsuneyama, K; Saito K; Ruebner BH; Konishi I; Nakanuma Y; Gershwin ME (2000). "Immunological similarities between primary sclerosing cholangitis and chronic sclerosing sialadenitisreport of the overlapping of these two autoimmune diseases". Digestive Diseases and Sciences. 45 (2): 366–372. doi:10.1023/A:1005429130150. PMID 10711453. S2CID 24581402.
- ↑ Sekine, S; Nagata M; Watanabe T (1999). "Chronic sclerosing sialadenitis of the submandibular gland associated with idiopathic retroperitoneal fibrosis". Pathology International. 49 (7): 663–667. doi:10.1046/j.1440-1827.1999.00926.x. PMID 10504530. S2CID 21548017.
- 1 2 Kamisawa, T; Nakajima H; Hishima T (2006). "Close correlation between chronic sclerosing sialadenitis and immunoglobulin G4". Internal Medicine Journal. 36 (8): 527–529. doi:10.1111/j.1445-5994.2006.01119.x. PMID 16866659. S2CID 33328260.
- 1 2 Nagai, K; Andoh K; Ogata A; Aoki N; Nakamura N; Hosaka H; Kurihara R (2010). "A new category for chronic sclerosing sialadenitis as an IgG4 related syndrome". BMJ Case Reports. 2010: bcr1020092412. doi:10.1136/bcr.10.2009.2412. PMC 3028012 . PMID 22448185.
- ↑ Cheuk, W; Yuen HK; Chu SY; Chiu EK; Lam LK; Chan JK (2008). "Lymphadenopathy of IgG4-related sclerosing disease". Am J Surg Pathol. 32 (5): 671–681. doi:10.1097/PAS.0b013e318157c068. PMID 18344866. S2CID 27175700.
- ↑ Melo, JC; Kitsko D; Reyes-Múgica M (2012). "Pediatric chronic sclerosing sialadenitis: Küttner tumor". Pediatric and Developmental Pathology. 15 (2): 165–169. doi:10.2350/11-04-1023-OA.1. PMID 21985393. S2CID 26785007.
- 1 2 Chow, TL; Chan TT; Choi CY; Lam SH (2008). "Kuttner's tumour (chronic sclerosing sialadenitis) of the submandibular gland: a clinical perspective" (PDF). Hong Kong Medical Journal. 14 (1): 46–9. PMID 18239243 . Retrieved 15 November 2013.
- 1 2 Chou, YH; Tiu CM; Li WY; Liu CY; Cheng YC; Chiou HJ; Chiou SY; Wang HK; Hung GS (2005). "Chronic sclerosing sialadenitis of the parotid gland: diagnosis using color Doppler sonography and sonographically guided needle biopsy". Journal of Ultrasound in Medicine. 24 (4): 551–555. doi: 10.7863/jum.2005.24.4.551 . PMID 15784774. S2CID 24563080 . Retrieved 17 November 2013.
- ↑ Cheuk, W; Chan, JKC (2002). "Kuttner Tumor of the Submandibular Gland: Fine-Needle Aspiration Cytologic Findings of Seven Case" (PDF). American Journal of Clinical Pathology. 117 (1): 103–108. doi: 10.1309/g9t3-22mh-q7kl-g2dl . PMID 11791589 . Retrieved 5 December 2013.
- 1 2 Abu, A; Motoori K; Yamamoto S; Hanazawa T; Nagai Y; Kaneoya K; Ito H (2008). "MRI of chronic sclerosing sialoadenitis". British Journal of Radiology. 81 (967): 531–536. doi:10.1259/bjr/38960620. PMID 18316344.