
Human teeth function to mechanically break down items of food by cutting and crushing them in preparation for swallowing and digesting. As such, they are considered part of the human digestive system. Humans have four types of teeth: incisors, canines, premolars, and molars, which each have a specific function. The incisors cut the food, the canines tear the food and the molars and premolars crush the food. The roots of teeth are embedded in the maxilla or the mandible and are covered by gums. Teeth are made of multiple tissues of varying density and hardness.

Toothache, also known as dental pain or tooth pain, is pain in the teeth or their supporting structures, caused by dental diseases or pain referred to the teeth by non-dental diseases. When severe it may impact sleep, eating, and other daily activities.

The pulp is the connective tissue, nerves, blood vessels, and odontoblasts that comprise the innermost layer of a tooth. The pulp's activity and signalling processes regulate its behaviour.

Tooth development or odontogenesis is the complex process by which teeth form from embryonic cells, grow, and erupt into the mouth. For human teeth to have a healthy oral environment, all parts of the tooth must develop during appropriate stages of fetal development. Primary (baby) teeth start to form between the sixth and eighth week of prenatal development, and permanent teeth begin to form in the twentieth week. If teeth do not start to develop at or near these times, they will not develop at all, resulting in hypodontia or anodontia.
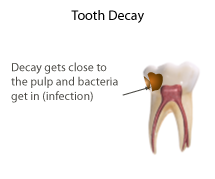
Pulpitis is inflammation of dental pulp tissue. The pulp contains the blood vessels, the nerves, and connective tissue inside a tooth and provides the tooth's blood and nutrients. Pulpitis is mainly caused by bacterial infection which itself is a secondary development of caries. It manifests itself in the form of a toothache.
A dental emergency is an issue involving the teeth and supporting tissues that are of high importance to be treated by the relevant professional. Dental emergencies do not always involve pain, although this is a common signal that something needs to be looked at. Pain can originate from the tooth, surrounding tissues or can have the sensation of originating in the teeth but be caused by an independent source. Depending on the type of pain experienced an experienced clinician can determine the likely cause and can treat the issue as each tissue type gives different messages in a dental emergency.

Veterinary dentistry is the field of dentistry applied to the care of animals. It is the art and science of prevention, diagnosis, and treatment of conditions, diseases, and disorders of the oral cavity, the maxillofacial region, and its associated structures as it relates to animals.
Dentin hypersensitivity is dental pain which is sharp in character and of short duration, arising from exposed dentin surfaces in response to stimuli, typically thermal, evaporative, tactile, osmotic, chemical or electrical; and which cannot be ascribed to any other dental disease.
Concrescence is an uncommon developmental condition of teeth where the cementum overlying the roots of at least two teeth fuse together without the involvement of dentin. Usually, two teeth are involved with the upper second and third molars being most commonly fused together. The prevalence ranges 0.04–0.8% in permanent teeth, with the incidence being highest in the posterior maxilla.
Dens invaginatus (DI), also known as tooth within a tooth, is a rare dental malformation and a developmental anomaly where there is an infolding of enamel into dentin. The prevalence of this condition is 0.3 - 10%, affecting males more frequently than females. The condition presents in two forms, coronal involving tooth crown and radicular involving tooth root, with the former being more common.
Dens evaginatus is a rare odontogenic developmental anomaly that is found in teeth where the outer surface appears to form an extra bump or cusp.
Talon cusp is a rare dental anomaly resulting in an extra cusp or cusp-like projection on an anterior tooth, located on the inside surface of the affected tooth. Sometimes it can also be found on the facial surface of the anterior tooth.

Dental attrition is a type of tooth wear caused by tooth-to-tooth contact, resulting in loss of tooth tissue, usually starting at the incisal or occlusal surfaces. Tooth wear is a physiological process and is commonly seen as a normal part of aging. Advanced and excessive wear and tooth surface loss can be defined as pathological in nature, requiring intervention by a dental practitioner. The pathological wear of the tooth surface can be caused by bruxism, which is clenching and grinding of the teeth. If the attrition is severe, the enamel can be completely worn away leaving underlying dentin exposed, resulting in an increased risk of dental caries and dentin hypersensitivity. It is best to identify pathological attrition at an early stage to prevent unnecessary loss of tooth structure as enamel does not regenerate.
Dental anatomy is a field of anatomy dedicated to the study of human tooth structures. The development, appearance, and classification of teeth fall within its purview. Tooth formation begins before birth, and the teeth's eventual morphology is dictated during this time. Dental anatomy is also a taxonomical science: it is concerned with the naming of teeth and the structures of which they are made, this information serving a practical purpose in dental treatment.
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.

Root canal treatment is a treatment sequence for the infected pulp of a tooth which is intended to result in the elimination of infection and the protection of the decontaminated tooth from future microbial invasion. Root canals, and their associated pulp chamber, are the physical hollows within a tooth that are naturally inhabited by nerve tissue, blood vessels and other cellular entities. Together, these items constitute the dental pulp.
Dental pertains to the teeth, including dentistry. Topics related to the dentistry, the human mouth and teeth include:

Barodontalgia, commonly known as tooth squeeze, is a pain in a tooth caused by a change in ambient pressure. The pain usually ceases at ground level. Dental barotrauma is a condition in which such changes in barometric pressure changes cause damage to the dentition.
Pulpotomy is a minimally invasive procedure performed in children on a primary tooth with extensive caries but without evidence of root pathology. The minimally invasive endodontic techniques of vital pulp therapy (VPT) are based on improved understanding of the capacity of pulp (nerve) tissues to heal and regenerate plus the availability of advanced endodontic materials. During the caries removal, this results in a carious or mechanical pulp exposure (bleeding) from the cavity. During pulpotomy, the inflamed/diseased pulp tissue is removed from the coronal pulp chamber of the tooth leaving healthy pulp tissue which is dressed with a long-term clinically successful medicament that maintains the survival of the pulp and promotes repair. There are various types of medicament placed above the vital pulp such as Buckley's Solution of formocresol, ferric sulfate, calcium hydroxide or mineral trioxide aggregate (MTA). MTA is a more recent material used for pulpotomies with a high rate of success, better than formocresol or ferric sulfate. It is also recommended to be the preferred pulpotomy agent in the future. After the coronal pulp chamber is filled, the tooth is restored with a filling material that seals the tooth from microleakage, such as a stainless steel crown which is the most effective long-term restoration. However, if there is sufficient remaining supporting tooth structure, other filling materials such as amalgam or composite resin can provide a functional alternative when the primary tooth has a life span of two years or less. The medium- to long-term treatment outcomes of pulpotomy in symptomatic permanent teeth with caries, especially in young people, indicate that pulpotomy can be a potential alternative to root canal therapy (RCT).

Pulp stones are nodular, calcified masses appearing in either or both the coronal and root portion of the pulp organ in teeth. Pulp stones are not painful unless they impinge on nerves.




