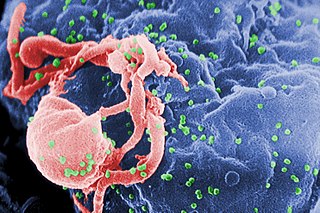
The human immunodeficiency viruses (HIV) are two species of Lentivirus that infect humans. Over time, they cause acquired immunodeficiency syndrome (AIDS), a condition in which progressive failure of the immune system allows life-threatening opportunistic infections and cancers to thrive. Without treatment, the average survival time after infection with HIV is estimated to be 9 to 11 years, depending on the HIV subtype.
Peter Heinz Hermann Duesberg is a German-American molecular biologist and a professor of molecular and cell biology at the University of California, Berkeley. He is known for his early research into the genetic aspects of cancer. He is a proponent of AIDS denialism, the claim that HIV does not cause AIDS.
Various fringe theories have arisen to speculate about purported alternative origins for the human immunodeficiency virus (HIV) and the acquired immunodeficiency syndrome (AIDS), with claims ranging from it being due to accidental exposure to supposedly purposeful acts. Several inquiries and investigations have been carried out as a result, and each of these theories has consequently been determined to be based on unfounded and/or false information. HIV has been shown to have evolved from or be closely related to the simian immunodeficiency virus (SIV) in West Central Africa sometime in the early 20th century. HIV was discovered in the 1980s by the French scientist Luc Montagnier. Before the 1980s, HIV was an unknown deadly disease.
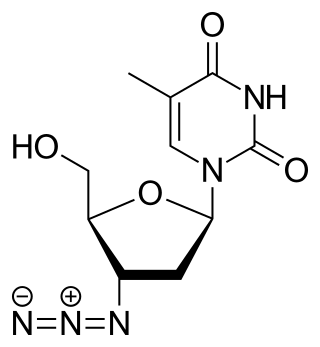
Zidovudine (ZDV), also known as azidothymidine (AZT), was the first antiretroviral medication used to prevent and treat HIV/AIDS. It is generally recommended for use in combination with other antiretrovirals. It may be used to prevent mother-to-child spread during birth or after a needlestick injury or other potential exposure. It is sold both by itself and together as lamivudine/zidovudine and abacavir/lamivudine/zidovudine. It can be used by mouth or by slow injection into a vein.

HIV/AIDS denialism is the belief, despite conclusive evidence to the contrary, that the human immunodeficiency virus (HIV) does not cause acquired immune deficiency syndrome (AIDS). Some of its proponents reject the existence of HIV, while others accept that HIV exists but argue that it is a harmless passenger virus and not the cause of AIDS. Insofar as they acknowledge AIDS as a real disease, they attribute it to some combination of sexual behavior, recreational drugs, malnutrition, poor sanitation, haemophilia, or the effects of the medications used to treat HIV infection (antiretrovirals).
The spread of HIV/AIDS has affected millions of people worldwide; AIDS is considered a pandemic. The World Health Organization (WHO) estimated that in 2016 there were 36.7 million people worldwide living with HIV/AIDS, with 1.8 million new HIV infections per year and 1 million deaths due to AIDS. Misconceptions about HIV and AIDS arise from several different sources, from simple ignorance and misunderstandings about scientific knowledge regarding HIV infections and the cause of AIDS to misinformation propagated by individuals and groups with ideological stances that deny a causative relationship between HIV infection and the development of AIDS. Below is a list and explanations of some common misconceptions and their rebuttals.

Kaposi's sarcoma-associated herpesvirus (KSHV) is the ninth known human herpesvirus; its formal name according to the International Committee on Taxonomy of Viruses (ICTV) is Human gammaherpesvirus 8, or HHV-8 in short. Like other herpesviruses, its informal names are used interchangeably with its formal ICTV name. This virus causes Kaposi's sarcoma, a cancer commonly occurring in AIDS patients, as well as primary effusion lymphoma, HHV-8-associated multicentric Castleman's disease and KSHV inflammatory cytokine syndrome. It is one of seven currently known human cancer viruses, or oncoviruses. Even after many years since the discovery of KSHV/HHV8, there is no known cure for KSHV associated tumorigenesis.
This is a timeline of HIV/AIDS, including but not limited to cases before 1980.

An opportunistic infection is an infection caused by pathogens that take advantage of an opportunity not normally available. These opportunities can stem from a variety of sources, such as a weakened immune system, an altered microbiome, or breached integumentary barriers. Many of these pathogens do not necessarily cause disease in a healthy host that has a non-compromised immune system, and can, in some cases, act as commensals until the balance of the immune system is disrupted. Opportunistic infections can also be attributed to pathogens which cause mild illness in healthy individuals but lead to more serious illness when given the opportunity to take advantage of an immunocompromised host.
AIDS-defining clinical conditions is the list of diseases published by the Centers for Disease Control and Prevention (CDC) that are associated with AIDS and used worldwide as a guideline for AIDS diagnosis. CDC exclusively uses the term AIDS-defining clinical conditions, but the other terms remain in common use.
AIDS is caused by a human immunodeficiency virus (HIV), which originated in non-human primates in Central and West Africa. While various sub-groups of the virus acquired human infectivity at different times, the present pandemic had its origins in the emergence of one specific strain – HIV-1 subgroup M – in Léopoldville in the Belgian Congo in the 1920s.
A passenger virus is a virus that is frequently found in samples from diseased tissue, such as tumours, but is not a contributing factor in causing the disease.

Patrick S. Moore is an American virologist and epidemiologist who co-discovered together with his wife, Yuan Chang, two different human viruses causing the AIDS-related cancer Kaposi's sarcoma and the skin cancer Merkel cell carcinoma. Moore and Chang have discovered two of the seven known human viruses causing cancer. The couple met while in medical school together and were married in 1989 while they pursued fellowships at different universities.

The human immunodeficiency virus (HIV) is a retrovirus that attacks the immune system. It is a preventable disease. There is no vaccine or cure for HIV. It can be managed with treatment and become a manageable chronic health condition. While there is no cure or vaccine, antiretroviral treatment can slow the course of the disease and enable people living with HIV to lead long and healthy lives. An HIV-positive person on treatment can expect to live a normal life, and die with the virus, not of it. Effective treatment for HIV-positive people involves a life-long regimen of medicine to suppress the virus, making the viral load undetectable. Without treatment it can lead to a spectrum of conditions including acquired immunodeficiency syndrome (AIDS).

The Democratic Republic of the Congo was one of the first African countries to recognize HIV, registering cases of HIV among hospital patients as early as 1983.

With an estimated 150,000 people living with HIV/AIDS in 2016, Haiti has the most overall cases of HIV/AIDS in the Caribbean and its HIV prevalence rates among the highest percentage-wise in the region. There are many risk-factor groups for HIV infection in Haiti, with the most common ones including lower socioeconomic status, lower educational levels, risky behavior, and lower levels of awareness regarding HIV and its transmission.

Kaposi's sarcoma (KS) is a type of cancer that can form masses on the skin, in lymph nodes, in the mouth, or in other organs. The skin lesions are usually painless, purple and may be flat or raised. Lesions can occur singly, multiply in a limited area, or may be widespread. Depending on the sub-type of disease and level of immune suppression, KS may worsen either gradually or quickly. Except for Classical KS where there is generally no immune suppression, KS is caused by a combination of immune suppression and infection by Human herpesvirus 8.
Inventing the AIDS Virus is a 1996 book by molecular biologist Peter Duesberg, in which the author argues that HIV does not cause AIDS. Duesberg contends that HIV is a harmless passenger virus and that AIDS is caused by unrelated factors such as drug abuse, antiretroviral medication, chronic malnutrition, poor sanitation, and hemophilia. The unambiguous scientific consensus is that HIV causes AIDS and that Duesberg's claims are incorrect. Duesberg received a negative response from the scientific community for supporting AIDS denialism, misrepresenting and ignoring the scientific evidence that HIV causes AIDS, and for relying upon poor logic and manipulation. The book was also the subject of an authorship dispute with one of his graduate students.
Michael Stuart Gottlieb is an American physician and immunologist known for his 1981 identification of acquired immune deficiency syndrome (AIDS) as a new disease, and for his HIV/AIDS research, HIV/AIDS activism, and philanthropic efforts associated with HIV/AIDS treatment.

The stages of HIV infection are acute infection, latency, and AIDS. Acute infection lasts for several weeks and may include symptoms such as fever, swollen lymph nodes, inflammation of the throat, rash, muscle pain, malaise, and mouth and esophageal sores. The latency stage involves few or no symptoms and can last anywhere from two weeks to twenty years or more, depending on the individual. AIDS, the final stage of HIV infection, is defined by low CD4+ T cell counts, various opportunistic infections, cancers, and other conditions.

