Increased urination is a commonly reported side effect, particularly during the initial phase following treatment initiation; this is mostly transient and tends to reduce with sustained treatment. Common side effects for antimineralocorticoid medications include nausea and vomiting, stomach cramps and diarrhoea.[4] Clinically significant hyperkalemia is possible, and warrants serum potassium monitoring on a periodic basis. The pathophysiology of hyperkalemia is that antimineralocorticoid medications reduce potassium (K) excretion.
Mineralocorticoid receptor antagonists decrease the aldosterone effect by binding to the mineralocorticoid receptor inhibiting aldosterone. This leads to higher levels of potassium in serum and increased sodium excretion, resulting in decreased body fluid and lower blood pressure.[5]
When comparing the pharmacokinetic properties of spironolactone and eplerenone, it is clear that the two drugs differ. Spironolactone has shorter half-life (t1/2 = 1.3-1.4 hours) than eplerenone (t1/2 = 4–6 hours). Eplerenone goes through rapid metabolism by the liver to inactive metabolites (t1/2 = 4–6 hours). However, spironolactone is metabolized to three active metabolites, which give it prolonged activity (13.8 – 16. 5 hours). Spironolactone has a long half-life and is excreted 47-51% through kidneys. Patients with chronic kidney disease therefore require close monitoring when taking the drug. Spironolactone is also eliminated through feces (35-41%). The excretion of eplerenone is 67% through kidneys and 32% through feces. The information about excretion plays a critical role when determining the appropriate doses for patients with renal and/or hepatic dysfunction. It is very important to adjust the doses for patients with renal dysfunction because if they fail to eliminate the drug through their kidneys it could accumulate in the body, causing high concentration of potassium in the blood.[5]
Structure-activity relationship
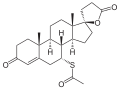
Spironolactone and Eplerenone competitively block the binding of aldosterone to the mineralocorticoid receptor and hindering the reabsorption of sodium and chloride ions. The activity of mineralocorticoid antagonists is dependent on the presence of a y-lactone ring on the C-17 position. The C-7 position is also important for activity as substituents there sterically hinder the interaction of C-7-unsubstituted agonists such as aldosterone.[7]
Antimineralocorticoids and highlighted groups that are important for activity. The y-lactone ring shown in red and the C-7 substituent in pink.
Despite the nonsteroidal nature of finerenone which yields a different lipophilicity and polarity profile for this compound, finerenone's affinity toward mineralocorticoid receptors is equal to that of spironolactone and 500 times that of eplerenone, hinting that the steroidal core component of most antimineralocorticoids is not essential for mineralocorticoid receptor affinity.[8]
History
The main goal of the identification of the first aldosterone antagonists, which happened during the 1950s, was to identify inhibitors of aldosterone activity. In those times, the main use of aldosterone was recognized as the control of renal sodium and the excretion of potassium.[8]
Hans Selye, a Hungarian-Canadian endocrinologist, studied the effects of aldosterone antagonists on rats and found that the use of one of the first aldosterone antagonists, spironolactone, protected them from aldosterone-induced cardiac necrosis. The same year, 1959, spironolactone was launched as a potassium-sparing diuretic. It became clear years later that aldosterone antagonists inhibit a specific receptor protein. This protein has high affinity for aldosterone but also for cortisol in humans and corticosterone in mice and rats. For this reason, aldosterone antagonists were called mineralocorticoid receptor antagonists.[8]
Around 50 years after Selye's work, several pharmaceutical companies began drug discovery programs. Their goal was to discover novel non-steroidal mineralocorticoid receptor antagonists for use as efficacious and safe drugs with the pharmacodynamics and pharmacokinetics well defined. Their goal was to use these candidates for a broad spectrum of diseases. This was essentially the third wave. The first mineralocorticoid receptor antagonists were all discovered and identified by in vivo experiments whereas the identification of novel non-steroidal mineralocorticoid receptor antagonists were done with high-throughput screening of millions of chemical compounds in various pharmaceutical companies.[8]
↑ The Krause/King-Lewis acronym, developed at Naval Medical Center San DiegoArchived 2018-07-13 at the Wayback Machine , of MCRA was developed during February 2017 to distinguish between MRA for a specific MRI which are both widely recognized medical acronyms as compared to the use of MRA for mineralocorticoid receptor antagonist type medications which is only used as a medical acronym in the cardiology and nephrology word.
1 2 Lemke, Thomas L.; Williams, David A.; Roche, Victoria F.; Zito, S. William. Foye's Principals of Medicinal Chemistry. Wolters Kluwer - Lippincott Williams and Wilkins.
↑ Kosaka H, Hirayama K, Yoda N, Sasaki K, Kitayama T, Kusaka H, Matsubara M (2010). "The L-, N-, and T-type triple calcium channel blocker benidipine acts as an antagonist of mineralocorticoid receptor, a member of nuclear receptor family". Eur. J. Pharmacol. 635 (1–3): 49–55. doi:10.1016/j.ejphar.2010.03.018. PMID20307534.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.