Tetanus, also known as lockjaw, is a bacterial infection caused by Clostridium tetani and characterized by muscle spasms. In the most common type, the spasms begin in the jaw, and then progress to the rest of the body. Each spasm usually lasts for a few minutes. Spasms occur frequently for three to four weeks.[1] Some spasms may be severe enough to fracture bones.[2] Other symptoms of tetanus may include fever, sweating, headache, trouble swallowing, high blood pressure, and a fast heart rate. Onset of symptoms is typically 3 to 21 days following infection. Recovery may take months; about 10% of cases prove to be fatal.[1]
C. tetani is commonly found in soil, saliva, dust, and manure. The bacteria generally enter through a break in the skin, such as a cut or puncture wound caused by a contaminated object.[1][3] They produce toxins that interfere with normal muscle contractions.[4] Diagnosis is based on the presenting signs and symptoms. The disease does not spread between people.[1]
Tetanus can be prevented by immunization with the tetanus vaccine. In those who have a significant wound and have had fewer than three doses of the vaccine, both vaccination and tetanus immune globulin are recommended. The wound should be cleaned, and any dead tissue should be removed. In those who are infected, tetanus immune globulin, or, if unavailable, intravenous immunoglobulin (IVIG) is used.[1]Muscle relaxants may be used to control spasms. Mechanical ventilation may be required if a person's breathing is affected.[4]
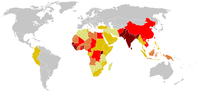
Tetanus occurs in all parts of the world, but is most frequent in hot and wet climates where the soil has a high organic content.[1] In 2015, there were about 209,000 infections and about 59,000 deaths globally.[5][6] This is down from 356,000 deaths in 1990.[7] In the US, there are about 30 cases per year, almost all of which were in people who had not been vaccinated.[8] An early description of the disease was made by Hippocrates in the 5th century BC. The cause of the disease was determined in 1884 by Antonio Carle and Giorgio Rattone at the University of Turin, and a vaccine was developed in 1924.[1]
Even with treatment, about 10% of people who contract tetanus die.[1] The mortality rate is higher in unvaccinated individuals, and in people over 60 years of age.[1]
Incubation period
The incubation period of tetanus may be up to several months, but is usually about ten days.[12][13] In general, the farther the injury site is from the central nervous system, the longer the incubation period. However, shorter incubation periods will have more severe symptoms.[14] In trismus nascentium (i.e. neonatal tetanus), symptoms usually appear from 4 to 14 days after birth, averaging about 7 days. On the basis of clinical findings, four different forms of tetanus have been described.[1]
Generalized tetanus
Generalized tetanus is the most common type of tetanus, representing about 80% of cases. The generalized form usually presents with a descending pattern. The first sign is trismus or lockjaw, then facial spasms (called risus sardonicus), followed by stiffness of the neck, difficulty in swallowing, and rigidity of pectoral and calf muscles. Other symptoms include elevated temperature, sweating, elevated blood pressure, and episodic rapid heart rate. Spasms may occur frequently and last for several minutes, with the body shaped into a characteristic form called opisthotonos. Spasms continue for up to four weeks, and complete recovery may take months.[1]
Neonatal tetanus (trismus nascentium) is a form of generalized tetanus that occurs in newborns, usually those born to mothers who themselves have not been vaccinated. If the mother has been vaccinated against tetanus, the infants acquire passive immunity, and are thus protected.[15] It usually occurs through infection of the unhealed umbilical stump, particularly when the stump is cut with a non-sterile instrument. As of 1998, neonatal tetanus was common in many developing countries, and was responsible for about 14% (215,000) of all neonatal deaths.[16] In 2010, the worldwide death toll was approximately 58,000 newborns. As the result of a public health campaign, the death toll from neonatal tetanus was reduced by 90% between 1990 and 2010, and by 2013, the disease had been largely eliminated from all but 25 countries.[17] Neonatal tetanus is rare in developed countries.
Local tetanus
Local tetanus is an uncommon form of the disease, in which people have persistent contraction of muscles in the same anatomic area as the injury. The contractions may persist for many weeks before gradually subsiding. Local tetanus is generally milder; only about 1% of cases are fatal, but it may precede the onset of generalized tetanus.[1]
Cephalic tetanus
Cephalic tetanus is the rarest form of the disease (0.9–3% of cases),[18] and is limited to muscles and nerves in the head.[19] It usually occurs after trauma to the head area, including: skull fracture,[20] laceration,[20] eye injury,[19]dental extraction,[21] and otitis media,[22] but it has been observed from injuries to other parts of the body.[23] Paralysis of the facial nerve is most frequently implicated, which may cause lockjaw, facial palsy, or ptosis, but other cranial nerves can also be affected.[21][24] Cephalic tetanus may progress to a more generalized form of the disease.[18][24] Due to its rarity, clinicians may be unfamiliar with the clinical presentation, and may not suspect tetanus as the illness.[19] Treatment can be complicated, as symptoms may be concurrent with the initial injury that caused the infection.[20] Cephalic tetanus is more likely than other forms of tetanus to be fatal, with the progression to generalized tetanus carrying a 15–30% case fatality rate.[18][20][24]
Cause
Clostridium tetani is durable due to its endospores. Pictured is the bacterium alone, with a spore being produced, and the spore alone.
Tetanus is caused by the tetanus bacterium, Clostridium tetani.[1] The disease is an international health problem, as C.tetaniendospores are ubiquitous. Endospores can be introduced into the body through a puncture wound (penetrating trauma). Due to C.tetani being an anaerobic bacterium, it and its endospores thrive in environments that lack oxygen, such as a puncture wound. With the changes in oxygen levels, the drumstick-shaped endospore can quickly spread.[25]
The disease occurs almost exclusively in people who are inadequately immunized.[26] It is more common in hot, damp climates with soil rich in organic matter. Manure-treated soils may contain spores, as they are widely distributed in the intestines and feces of many animals, such as horses, sheep, cattle, dogs, cats, rats, guinea pigs, and chickens.[1] In agricultural areas, a significant number of human adults may harbor the organism.[27]
The spores can also be found on skin surfaces and in contaminated heroin.[1] Rarely, tetanus can be contracted through surgical procedures, intramuscular injections, compound fractures, and dental infections.[1] Animal bites can transmit tetanus.[1]
Tetanus is often associated with rust, especially rusty nails. Although rust itself does not cause tetanus, objects that accumulate rust are often found outdoors or in places that harbor anaerobic bacteria. Additionally, the rough surface of rusty metal provides crevices for dirt containing C.tetani, while a nail affords a means to puncture skin and deliver endospores deep within the body at the site of the wound.[28] An endospore is a non-metabolizing survival structure that begins to metabolize and cause infection once in an adequate environment. Hence, stepping on a nail (rusty or not) may result in a tetanus infection, as the low-oxygen (anaerobic) environment may exist under the skin, and the puncturing object can deliver endospores to a suitable environment for growth.[29] It is a common misconception that rust itself is the cause, and that a puncture from a rust-free nail is not a risk.[30][31]
Pathophysiology
A neurotransmitter-filled vesicle before and after exposure to the tetanus toxin. The cleavage of the VAMP protein by the toxin inhibits vesicle fusion and neurotransmitter release into the synapse.
Tetanus neurotoxin (TeNT) binds to the presynaptic membrane of the neuromuscular junction, is internalized, and is transported back through the axon until it reaches the central nervous system.[32] Here, it selectively binds to and is transported into inhibitory neurons via endocytosis.[33] It then leaves the vesicle for the neuron cytosol, where it cleaves vesicle associated membrane protein (VAMP) synaptobrevin, which is necessary for membrane fusion of small synaptic vesicles (SSV's).[32] SSV's carry neurotransmitter to the membrane for release, so inhibition of this process blocks neurotransmitter release.[citation needed]
Tetanus toxin specifically blocks the release of the neurotransmitters GABA and glycine from inhibitory neurons. These neurotransmitters keep overactive motor neurons from firing, and also play a role in the relaxation of muscles after contraction. When inhibitory neurons are unable to release their neurotransmitters, motor neurons fire out of control, and muscles have difficulty relaxing. This causes the muscle spasms and spastic paralysis seen in tetanus infection.[32]
The tetanus toxin, tetanospasmin, is made up of a heavy chain and a light chain. There are three domains, each of which contributes to the pathophysiology of the toxin.[34] The heavy chain has two of the domains. The N-terminal side of the heavy chain helps with membrane translocation, and the C-terminal side helps the toxin locate the specific receptor site on the correct neuron. The light chain domain cleaves the VAMP protein once it arrives in the inhibitory neuron cytosol.[34]
There are four main steps in tetanus's mechanism of action: binding to the neuron, internalization of the toxin, membrane translocation, and cleavage of the target VAMP.[35]
Neurospecific binding
The toxin travels from the wound site to the neuromuscular junction through the bloodstream, where it binds to the presynaptic membrane of a motor neuron. The heavy chain C-terminal domain aids in the binding to the correct site, recognizing and binding to the correct glycoproteins and glycolipids in the presynaptic membrane. The toxin binds to a site that will be taken into the neuron as an endocytic vesicle that will travel down the axon, past the cell body, and down the dendrites to the dendritic terminal at the spine and central nervous system. Here, it will be released into the synaptic cleft, and allowed to bind with the presynaptic membrane of inhibitory neurons in a similar manner seen with the binding to the motor neuron.[33]
Internalization
Tetanus toxin is then internalized again via endocytosis, this time, in an acidic vesicle.[34] In a mechanism not well understood, depolarization caused by the firing of the inhibitory neuron causes the toxin to be pulled into the neuron inside vesicles.[citation needed]
Membrane translocation
The toxin then needs a way to get out of the vesicle and into the neuron cytosol for it to act on its target. The low pH of the vesicle lumen causes a conformational change in the toxin, shifting it from a water-soluble form to a hydrophobic form.[33] With the hydrophobic patches exposed, the toxin can slide into the vesicle membrane. The toxin forms an ion channel in the membrane that is nonspecific for Na+, K+, Ca2+, and Cl− ions.[32] There is a consensus among experts that this new channel is involved in the translocation of the toxin's light chain from the inside of the vesicle to the neuron cytosol, but the mechanism is not well understood or agreed upon. It has been proposed that the channel could allow the light chain (unfolded from the low pH environment) to leave through the toxin pore,[36] or that the pore could alter the electrochemical gradient enough, by letting in or out ions, to cause osmotic lysis of the vesicle, spilling the vesicle's contents.[37]
Enzymatic target cleavage
The light chain of the tetanus toxin is zinc-dependent protease. It shares a common zinc protease motif (His-Glu-Xaa-Xaa-His) that researchers hypothesized was essential for target cleavage, until this was more recently confirmed by experiment: when all zinc was removed from the neuron with heavy metal chelators, the toxin was inhibited, only to be reactivated when the zinc was added back in.[32] The light chain binds to VAMP, and cleaves it between Gln76 and Phe77. Without VAMP, vesicles holding the neurotransmitters needed for motor neuron regulation (GABA and glycine) cannot be released, causing the above-mentioned deregulation of motor neurons and muscle tension.[38]
Diagnosis
There are currently no blood tests for diagnosing tetanus. The diagnosis is based on the presentation of tetanus symptoms, and does not depend upon isolation of the bacterium, which is recovered from the wound in only 30% of cases, and can be isolated from people without tetanus. Laboratory identification of C.tetani can be demonstrated only by production of tetanospasmin in mice.[1] Having recently experienced head trauma may indicate cephalic tetanus if no other diagnosis has been made.[citation needed]
The "spatula test" is a clinical test for tetanus that involves touching the posteriorpharyngeal wall with a soft-tipped instrument and observing the effect. A positive test result is the involuntary contraction of the jaw (biting down on the "spatula"), and a negative test result would normally be a gag reflex attempting to expel the foreign object. A short report in The American Journal of Tropical Medicine and Hygiene states that, in an affected subject research study, the spatula test had a high specificity (zero false-positive test results) and a high sensitivity (94% of infected people produced a positive test).[39]
Prevention
Unlike many infectious diseases, recovery from naturally acquired tetanus does not usually result in immunity. This is due to the extreme potency of the tetanospasmin toxin. Tetanospasmin will likely be lethal before it will provoke an immune response.[40]
Tetanus can be prevented by vaccination with tetanus toxoid.[41] The CDC recommends that adults receive a booster vaccine every ten years,[1] and standard care practice in many places is to give the booster to any person with a puncture wound who is uncertain of when he or she was last vaccinated, or if he or she has had fewer than three lifetime doses of the vaccine. The booster may not prevent a potentially fatal case of tetanus from the current wound, however, as it can take up to two weeks for tetanus antibodies to form.[42]
In children under the age of seven, the tetanus vaccine is often administered as a combined vaccine, DPT/DTaP vaccine, which also includes vaccines against diphtheria and pertussis. For adults and children over seven, the Td vaccine (tetanus and diphtheria) or Tdap (tetanus, diphtheria, and acellular pertussis) is commonly used.[41]
The World Health Organization certifies countries as having eliminated maternal or neonatal tetanus. Certification requires at least two years of rates of less than 1 case per 1,000 live births. In 1998 in Uganda, 3,433 tetanus cases were recorded in newborn babies; of these, 2,403 died. After a major public health effort, Uganda was certified as having eliminated maternal and neonatal tetanus in 2011.[43]
Severe cases will require admission to intensive care. In addition to the measures listed above for mild tetanus:[45]
Human tetanus immunoglobulin injected intrathecally (which increases clinical improvement from 4% to 35%).
Tracheotomy and mechanical ventilation for 3 to 4 weeks. Tracheotomy is recommended for securing the airway, because the presence of an endotracheal tube is a stimulus for spasm.
Magnesium sulfate, as an intravenous infusion, to control spasm and autonomic dysfunction.
Drugs, such as diazepam or other muscle relaxants, can be given to control the muscle spasms. In extreme cases, it may be necessary to paralyze the person with curare-like drugs, and use a mechanical ventilator.[citation needed]
To survive a tetanus infection, the maintenance of an airway and proper nutrition are required. An intake of 3,500 to 4,000 calories and at least 150g of protein per day is often given in liquid form through a tube directly into the stomach (percutaneous endoscopic gastrostomy), or through a drip into a vein (parenteral nutrition). This high-caloric diet maintenance is required because of the increased metabolic strain brought on by the increased muscle activity. Full recovery takes 4 to 6 weeks, because the body must regenerate destroyed nerve axon terminals.[citation needed]
The antibiotic of choice is metronidazole. It can be given as intravenously, by mouth, or by rectum.[46][45] Of likewise efficiency is penicillin, but some raise the concern of provoking spasms because it inhibits GABA receptor, which is already affected by tetanospasmin.[47]
In 2013, it caused about 59,000 deaths—down from 356,000 in 1990.[7] Tetanus, notably the neonatal form, remains a significant public health problem in non-industrialized countries, with 59,000 newborns dying worldwide in 2008 as a result of neonatal tetanus.[48][49] In the United States, from 2000 through 2007, an average of 31 cases were reported per year.[1] Nearly all of the cases in the United States occur in unimmunized individuals, or individuals who have allowed their inoculations to lapse.[1]
Tetanus cases reported worldwide (1990–2004). Ranging from some (in dark red), to very few (in light yellow) (grey, no data).
Tetanus deaths between 1990 and 2017 by age group.[50]
In animals
Tetanus is found primarily in goats and sheep. The following are clinical symptoms found in affected goats and sheep. Extended head and neck, tail rigors (tail becomes rigid and straight), abnormal gait (walking becomes stiff and abnormal), arched back, stiffness of the jaw muscles, lockjaw, twitching of eyes, drooping eyelids, difficulty swallowing, difficulty or inability to eat and drink, abdominal bloat, spasms (uncontrolled muscular contractions) before death. Death sometimes is due to asphyxiation, secondary to respiratory paralysis.[51]
History
Tetanus was well known to ancient civilizations, who recognized the relationship between wounds and fatal muscle spasms.[52] In 1884, Arthur Nicolaier isolated the strychnine-like toxin of tetanus from free-living, anaerobic soil bacteria. The etiology of the disease was further elucidated in 1884 by Antonio Carle and Giorgio Rattone, two pathologists of the University of Turin, who demonstrated the transmissibility of tetanus for the first time. They produced tetanus in rabbits by injecting pus from a person with fatal tetanus into their sciatic nerves, and testing their reactions while tetanus was spreading.[1]
In 1891, C.tetani was isolated from a human victim by Kitasato Shibasaburō, who later showed that the organism could produce disease when injected into animals, and that the toxin could be neutralized by specific antibodies. In 1897, Edmond Nocard showed that tetanus antitoxin induced passive immunity in humans, and could be used for prophylaxis and treatment. Tetanus toxoid vaccine was developed by P. Descombey in 1924, and was widely used to prevent tetanus induced by battle wounds during World War II.[1]
There is insufficient evidence that tetanus can be treated or prevented by vitamin C. This is at least partially due to the fact that the historical trials that were conducted in attempts to look for a possible connection between vitamin C and alleviating tetanus patients were of poor quality.[54]
Botulism is a rare and potentially fatal illness caused by a toxin produced by the bacterium Clostridium botulinum. The disease begins with weakness, blurred vision, feeling tired, and trouble speaking. This may then be followed by weakness of the arms, chest muscles, and legs. Vomiting, swelling of the abdomen, and diarrhea may also occur. The disease does not usually affect consciousness or cause a fever.
Diphtheria is an infection caused by the bacterium Corynebacterium diphtheriae. Most infections are asymptomatic or have a mild clinical course, but in some outbreaks, the mortality rate approaches 10%. Signs and symptoms may vary from mild to severe, and usually start two to five days after exposure. Symptoms often develop gradually, beginning with a sore throat and fever. In severe cases, a grey or white patch develops in the throat, which can block the airway, and create a barking cough similar to what is observed in croup. The neck may also swell, in part due to the enlargement of the facial lymph nodes. Diphtheria can also involve the skin, eyes, or genitals, and can cause complications, including myocarditis, inflammation of nerves, kidney problems, and bleeding problems due to low levels of platelets.
Tetanus toxin (TeNT) is an extremely potent neurotoxin produced by the vegetative cell of Clostridium tetani in anaerobic conditions, causing tetanus. It has no known function for clostridia in the soil environment where they are normally encountered. It is also called spasmogenic toxin, tentoxilysin, tetanospasmin or, tetanus neurotoxin. The LD50 of this toxin has been measured to be approximately 2.5–3 ng/kg, making it second only to the related botulinum toxin (LD50 2 ng/kg) as the deadliest toxin in the world. However, these tests are conducted solely on mice, which may react to the toxin differently from humans and other animals.
Trismus is a condition of restricted opening of the mouth. The term was initially used in the setting of tetanus. Trismus may be caused by spasm of the muscles of mastication or a variety of other causes. Temporary trismus occurs much more frequently than permanent trismus. It is known to interfere with eating, speaking, and maintaining proper oral hygiene. This interference, specifically with an inability to swallow properly, results in an increased risk of aspiration. In some instances, trismus presents with altered facial appearance. The condition may be distressing and painful. Examination and treatments requiring access to the oral cavity can be limited, or in some cases impossible, due to the nature of the condition itself.
In biology, immunity is the state of being insusceptible or resistant to a noxious agent or process, especially a pathogen or infectious disease. Immunity may occur naturally or be produced by prior exposure or immunization.
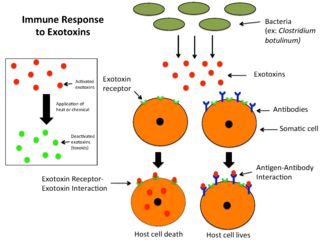
An exotoxin is a toxin secreted by bacteria. An exotoxin can cause damage to the host by destroying cells or disrupting normal cellular metabolism. They are highly potent and can cause major damage to the host. Exotoxins may be secreted, or, similar to endotoxins, may be released during lysis of the cell. Gram negative pathogens may secrete outer membrane vesicles containing lipopolysaccharide endotoxin and some virulence proteins in the bounding membrane along with some other toxins as intra-vesicular contents, thus adding a previously unforeseen dimension to the well-known eukaryote process of membrane vesicle trafficking, which is quite active at the host–pathogen interface.
A neuromuscular junction is a chemical synapse between a motor neuron and a muscle fiber.
The DPT vaccine or DTP vaccine is a class of combination vaccines against three infectious diseases in humans: diphtheria, pertussis, and tetanus (lockjaw). The vaccine components include diphtheria and tetanus toxoids, and either killed whole cells of the bacterium that causes pertussis or pertussis antigens. The term toxoid refers to vaccines which use an inactivated toxin produced by the pathogen which they are targeted against to generate an immune response. In this way, the toxoid vaccine generates an immune response which is targeted against the toxin which is produced by the pathogen and causes disease, rather than a vaccine which is targeted against the pathogen itself. The whole cells or antigens will be depicted as either "DTwP" or "DTaP", where the lower-case "w" indicates whole-cell inactivated pertussis and the lower-case "a" stands for "acellular". In comparison to alternative vaccine types, such as live attenuated vaccines, the DTP vaccine does not contain any live pathogen, but rather uses inactivated toxoid to generate an immune response; therefore, there is not a risk of use in populations that are immune compromised since there is not any known risk of causing the disease itself. As a result, the DTP vaccine is considered a safe vaccine to use in anyone and it generates a much more targeted immune response specific for the pathogen of interest.
The Clostridia are a highly polyphyletic class of Bacillota, including Clostridium and other similar genera. They are distinguished from the Bacilli by lacking aerobic respiration. They are obligate anaerobes and oxygen is toxic to them. Species of the class Clostridia are often but not always Gram-positive and have the ability to form spores. Studies show they are not a monophyletic group, and their relationships are not entirely certain. Currently, most are placed in a single order called Clostridiales, but this is not a natural group and is likely to be redefined in the future.
A toxoid is an inactivated toxin whose toxicity has been suppressed either by chemical (formalin) or heat treatment, while other properties, typically immunogenicity, are maintained. Toxins are secreted by bacteria, whereas toxoids are altered form of toxins; toxoids are not secreted by bacteria. Thus, when used during vaccination, an immune response is mounted and immunological memory is formed against the molecular markers of the toxoid without resulting in toxin-induced illness. Such a preparation is also known as an anatoxin. There are toxoids for prevention of diphtheria, tetanus and botulism.
The schedule for childhood immunizations in the United States is published by the Centers for Disease Control and Prevention (CDC). The vaccination schedule is broken down by age: birth to six years of age, seven to eighteen, and adults nineteen and older. Childhood immunizations are key in preventing diseases with epidemic potential.
Virulence factors are cellular structures, molecules and regulatory systems that enable microbial pathogens to achieve the following:
Tetany or tetanic seizure is a medical sign consisting of the involuntary contraction of muscles, which may be caused by disorders that increase the action potential frequency of muscle cells or the nerves that innervate them.
Flaccid paralysis is a neurological condition characterized by weakness or paralysis and reduced muscle tone without other obvious cause. This abnormal condition may be caused by disease or by trauma affecting the nerves associated with the involved muscles. For example, if the somatic nerves to a skeletal muscle are severed, then the muscle will exhibit flaccid paralysis. When muscles enter this state, they become limp and cannot contract. This condition can become fatal if it affects the respiratory muscles, posing the threat of suffocation. It also occurs in the spinal shock stage in complete transection of the spinal cord occurring in injuries such as gunshot wounds.
Immunization during pregnancy is the administration of a vaccine to a pregnant individual. This may be done either to protect the individual from disease or to induce an antibody response, such that the antibodies cross the placenta and provide passive immunity to the infant after birth. In many countries, including the US, Canada, UK, Australia and New Zealand, vaccination against influenza, COVID-19 and whooping cough is routinely offered during pregnancy.
Clostridium tetani is a common soil bacterium and the causative agent of tetanus. Vegetative cells of Clostridium tetani are usually rod-shaped and up to 2.5 μm long, but they become enlarged and tennis racket- or drumstick-shaped when forming spores. C. tetani spores are extremely hardy and can be found globally in soil or in the gastrointestinal tract of animals. If inoculated into a wound, C. tetani can grow and produce a potent toxin, tetanospasmin, which interferes with motor neurons, causing tetanus. The toxin's action can be prevented with tetanus toxoid vaccines, which are often administered to children worldwide.
Neonatal tetanus is a form of generalised tetanus that occurs in newborns. Infants who have not acquired passive immunity from an immunized mother are at risk. It usually occurs through infection of the unhealed umbilical stump, particularly when the stump is cut with a non-sterile instrument. Neonatal tetanus mostly occurs in developing countries, particularly those with the least developed health infrastructure. It is rare in developed countries.
Microbial toxins are toxins produced by micro-organisms, including bacteria, fungi, protozoa, dinoflagellates, and viruses. Many microbial toxins promote infection and disease by directly damaging host tissues and by disabling the immune system. Endotoxins most commonly refer to the lipopolysaccharide (LPS) or lipooligosaccharide (LOS) that are in the outer plasma membrane of Gram-negative bacteria. The botulinum toxin, which is primarily produced by Clostridium botulinum and less frequently by other Clostridium species, is the most toxic substance known in the world. However, microbial toxins also have important uses in medical science and research. Currently, new methods of detecting bacterial toxins are being developed to better isolate and understand these toxins. Potential applications of toxin research include combating microbial virulence, the development of novel anticancer drugs and other medicines, and the use of toxins as tools in neurobiology and cellular biology.
Tetanus vaccine, also known as tetanus toxoid (TT), is a toxoid vaccine used to prevent tetanus. During childhood, five doses are recommended, with a sixth given during adolescence.
DTaP-IPV-HepB vaccine is a combination vaccine whose generic name is diphtheria and tetanus toxoids and acellular pertussis adsorbed, hepatitis B (recombinant) and inactivated polio vaccine or DTaP-IPV-Hep B. It protects against the infectious diseases diphtheria, tetanus, pertussis, poliomyelitis, and hepatitis B.
↑ Schleiss MR (2020). "Chapter 238: Tetanus". In Kliegman, Robert (ed.). Nelson Textbook of Pediatrics. Elsevier. p.6253. ISBN978-0-323-52950-1.
↑ Vandelaer J, Birmingham M, Gasse F, Kurian M, Shaw C, Garnier S (July 2003). "Tetanus in developing countries: an update on the Maternal and Neonatal Tetanus Elimination Initiative". Vaccine. 21 (24): 3442–5. doi:10.1016/S0264-410X(03)00347-5. PMID12850356.
1 2 3 Del Pilar Morales E, Bertrán Pasarell J, Cardona Rodriguez Z, Almodovar Mercado JC, Figueroa Navarro A (2014). "Cephalic tetanus following penetrating eye trauma: a case report". Bol Asoc Med P R. 106 (2): 25–9. PMID25065047.
1 2 3 4 Adeleye AO, Azeez AL (October 2012). "Fatal tetanus complicating an untreated mild open head injury: a case-illustrated review of cephalic tetanus". Surgical Infections. 13 (5): 317–20. doi:10.1089/sur.2011.023. PMID23039234.
↑ Plumlee, Konnie H. (2004-01-01), Plumlee, Konnie H. (ed.), "Chapter 18 - Biotoxins", Clinical Veterinary Toxicology, Saint Louis: Mosby, pp.98–116, ISBN978-0-323-01125-9, retrieved 2022-06-21
↑ Beise J, Hahnen J, Andersen-Beckh B, Dreyer F (January 1994). "Pore formation by tetanus toxin, its chain, and fragments in neuronal membranes and evaluation of the underlying motifs in the structure of the toxin molecule". Naunyn-Schmiedeberg's Archives of Pharmacology. 349 (1): 66–73. doi:10.1007/BF00178208. PMID8139702. S2CID9398335.
↑ Cabiaux V, Lorge P, Vandenbranden M, Falmagne P, Ruysschaert JM (April 1985). "Tetanus toxin induces fusion and aggregation of lipid vesicles containing phosphatidylinositol at low pH". Biochemical and Biophysical Research Communications. 128 (2): 840–9. doi:10.1016/0006-291X(85)90123-8. PMID3994725.
↑ Foran P, Shone CC, Dolly JO (December 1994). "Differences in the protease activities of tetanus and botulinum B toxins revealed by the cleavage of vesicle-associated membrane protein and various sized fragments". Biochemistry. 33 (51): 15365–74. doi:10.1021/bi00255a017. PMID7803399.
↑ Apte NM, Karnad DR (October 1995). "Short Report: The Spatula Test: A Simple Bedside Test to Diagnose Tetanus". American Journal of Tropical Medicine and Hygiene. 53 (4): 386–7. doi:10.4269/ajtmh.1995.53.386. PMID7485691.
1 2 "Diphtheria, tetanus, and pertussis: recommendations for vaccine use and other preventive measures. Recommendations of the Immunization Practices Advisory committee (ACIP)". MMWR. Recommendations and Reports. 40 (RR-10): 1–28. August 1991. PMID1865873.
↑ Porter JD, Perkin MA, Corbel MJ, Farrington CP, Watkins JT, Begg NT (1992). "Lack of early antitoxin response to tetanus booster". Vaccine. 10 (5): 334–6. doi:10.1016/0264-410X(92)90373-R. PMID1574917.
↑ Thwaites, C. Louise; Yen, Lam Minh (13 August 2018). "Tetanus". In J. Larry Jameson (ed.). Harrison's Principles of Internal Medicine. Vol.1 and 2. Anthony S. Fauci, Dennis L. Kasper, Stephen L. Hauser, Dan L. Longo, Joseph Loscalzo (Twentiethed.). McGraw-Hill Education. p.2884. ISBN978-1-259-64403-0.
↑ Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, etal. (June 2010). "Global, regional, and national causes of child mortality in 2008: a systematic analysis". Lancet. 375 (9730): 1969–87. doi:10.1016/S0140-6736(10)60549-1. PMID20466419. S2CID27812760.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.