Calcitriol is a hormone and the active form of vitamin D, normally made in the kidney.[8][9][10] It is also known as 1,25-dihydroxycholecalciferol. It binds to and activates the vitamin D receptor in the nucleus of the cell, which then increases the expression of many genes.[11] Calcitriol increases blood calcium mainly by increasing the uptake of calcium from the intestines.[7]
Calcitriol was identified as the active form of vitamin D in 1971 and the drug was approved for medical use in the United States in 1978.[7] It is available as a generic medication.[12] In 2023, it was the 249th most commonly prescribed medication in the United States, with more than 1million prescriptions.[13][14] It is on the World Health Organization's List of Essential Medicines.[15]
Calcitriol has been used in an ointment for the treatment of psoriasis,[17] although the vitamin D analoguecalcipotriol (calcipotriene) is more commonly used.[18] Calcitriol has also been given by mouth for the treatment of psoriasis[19] and psoriatic arthritis.[20] Research on the noncalcemic actions of calcitriol and other VDR-ligand analogs and their possible therapeutic applications has been reviewed.[21]
High calcitriol levels may also be seen in human disease states in patients not on supplementation. In someone with hypercalcaemia and high calcitriol levels, low intact parathyroid hormone levels are usually present.
The major conditions with hypercalcaemia due to elevated calcitriol levels are lymphoma, tuberculosis and sarcoidosis where excess production occurs due to ectopic 25(OH)D-1-hydroxylase (CYP27B1) expressed in macrophages.[22] Other conditions producing similar findings including:
Some plants contain glycosides of 1,25-dihydroxycholecalciferol. Consumption of these glycosides by grazing animals leads to vitamin D toxicity, resulting in calcinosis, the deposition of excessive calcium in soft tissues. Three rangeland plants, Cestrum diurnum, Solanum malacoxylon, and Trisetum flavescens, are known to contain these glycosides. Of these, only C. diurnum is found in the U.S., mainly in Florida.[23]
Increasing renal tubular reabsorption of calcium, thus reducing the loss of calcium in the urine.
Stimulating release of calcium from bone. For this it acts on the specific type of bone cells referred to as osteoblasts, causing them to release RANKL, which in turn activates osteoclasts.[24]
Calcitriol acts in concert with parathyroid hormone (PTH) in all three of these roles. For instance, PTH also indirectly stimulates osteoclasts. However, the main effect of PTH is to increase the rate at which the kidneys excrete inorganic phosphate (Pi), the counterion of Ca2+ . The resulting decrease in serum phosphate causes hydroxyapatite (Ca5(PO4)3OH) to dissolve out of bone, thus increasing serum calcium. PTH also stimulates the production of calcitriol (see below).[25]
Many of the effects of calcitriol are mediated by its interaction with the calcitriol receptor, also called the vitamin D receptor or VDR.[26] For instance, the unbound inactive form of the calcitriol receptor in intestinal epithelial cells resides in the cytoplasm. When calcitriol binds to the receptor, the ligand-receptor complex translocates to the cell nucleus, where it acts as a transcription factor promoting the expression of a gene encoding a calcium binding protein. The levels of the calcium binding protein increase enabling the cells to actively transport more calcium (Ca2+ ) from the intestine across the intestinal mucosa into the blood.[25] Alternative, non-genomic pathways may be mediated through either PDIA3 or VDR.[27]
The maintenance of electroneutrality requires that the transport of Ca2+ ions catalyzed by the intestinal epithelial cells be accompanied by counterions, primarily inorganic phosphate. Thus calcitriol also stimulates the intestinal absorption of phosphate.[25]
The observation that calcitriol stimulates the release of calcium from bone seems contradictory, given that sufficient levels of serum calcitriol generally prevent overall loss of calcium from bone. It is believed that the increased levels of serum calcium resulting from calcitriol-stimulated intestinal uptake causes bone to take up more calcium than it loses by hormonal stimulation of osteoclasts.[25] Only when there are conditions, such as dietary calcium deficiency or defects in intestinal transport, which result in a reduction of serum calcium does an overall loss of calcium from bone occur.
Calcitriol also inhibits the release of calcitonin,[28] a hormone which reduces blood calcium primarily by inhibiting calcium release from bone.[25]
The activity of this enzyme is stimulated by PTH. This is an important control point in Ca2+ homeostasis.[25] Additional effects on the production of calcitriol include an increase by prolactin, a hormone which stimulates lactogenesis (the formation of milk in mammary glands), a process which requires large amounts of calcium.[29] Activity is also decreased by high levels of serum phosphate and by an increase in the production of the hormone FGF23 by osteocyte cells in bone.[30]
Calcitriol is also produced outside the kidney in small amounts by many other tissues including placenta and activated macrophages.[31]
When the drug alfacalcidol is used, 25-hydroxylation in the liver produces calcitriol as the active metabolite. This will produce greater effects than other vitamin D precursors in patients with kidney disease who have loss of the renal 1-alpha-hydroxylase.[32]
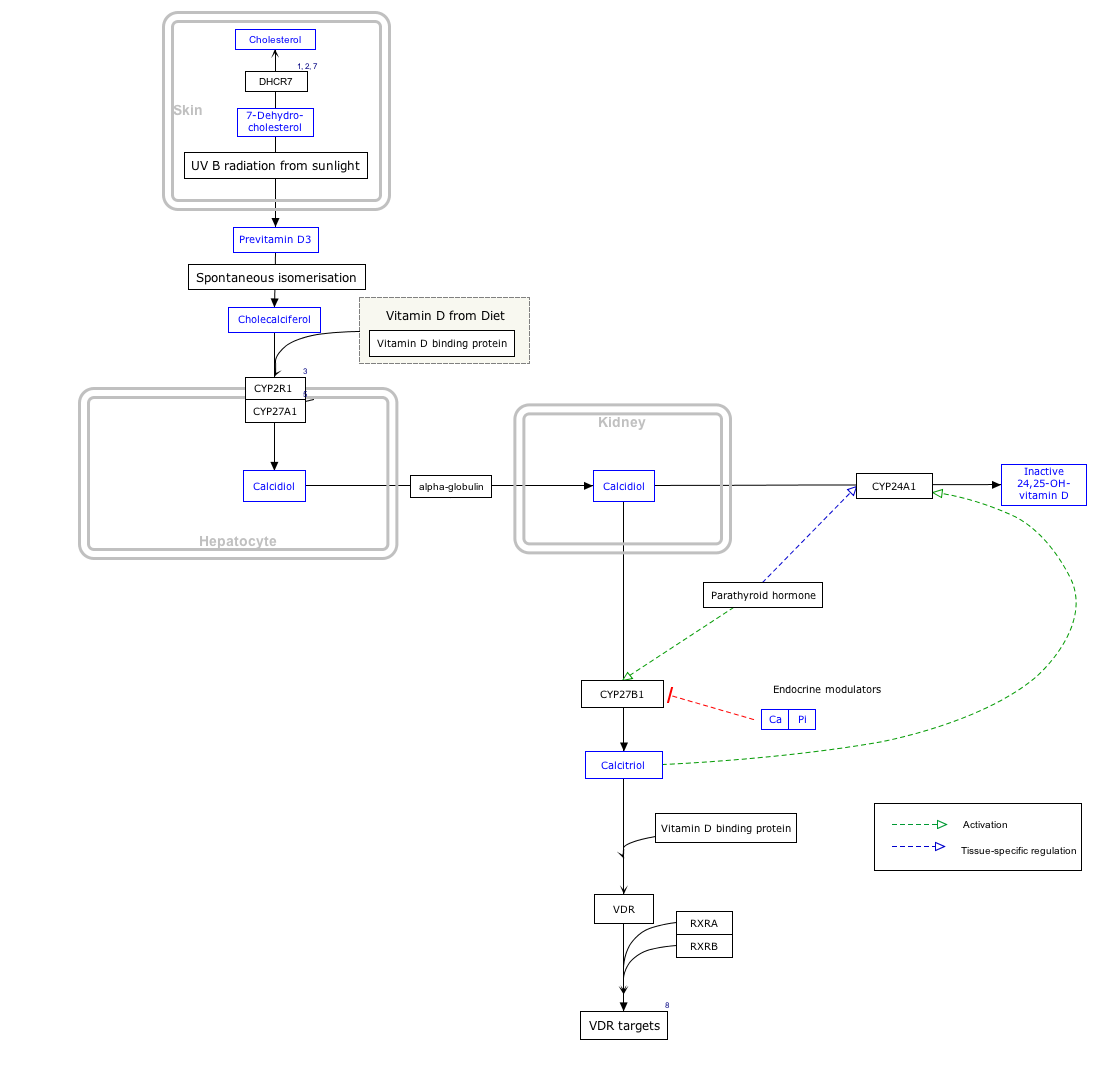
Interactive pathway map
Click on genes, proteins and metabolites below to link to respective articles.[§ 1]
half-life of calcitriol in the body has been reported between 3.5 hours[33] and 12–21 hours,[34] which is much shorter than that of its precursor calcifediol, whose half-life ranges have been estimated to range from about 15 days[35] and 21 days[36] to up to 149 days and 199 days.[37] Calcitriol is inactivated by further hydroxylation to form 1,24,25-trihydroxyvitamin D, calcitroic acid. This occurs through the action of the CYP24A1 24-hydroxylase.[38] Calcitroic acid is more soluble in water and is excreted in bile and urine.
It was approved for medical use in the United States in 1978.[7]
Names
Calcitriol refers specifically to 1,25-dihydroxycholecalciferol. Because cholecalciferol already has one hydroxyl group, only two (1,25) are further specified in this nomenclature, but in fact there are three (1,3,25-triol), as indicated by the name calcitriol. The 1-hydroxy group is in the alpha position, and this may be specified in the name, for instance in the abbreviation 1α,25-(OH)2D3.[6]
Calcitriol is, strictly, the 1-hydroxylation product of calcifediol (25-OH vitamin D3), derived from cholecalciferol (vitamin D3), rather than the product of hydroxylations of ergocalciferol (vitamin D2).[6] 1α,25-Dihydroxyergocalciferol (ercalcitriol) should be used for the vitamin D2 product.[6] However, the terminology of 1,25-dihydroxyvitamin D, or 1,25(OH)2D, is often used to refer to both types of active forms of vitamin D. Indeed, both bind to the vitamin D receptor and produce biological effects.[42] In clinical use, the differences are unlikely to have major importance.[32]
Calcitriol is marketed as a pharmaceutical for medical use under various brand names including Rocaltrol (Roche), Calcijex (Abbott), Decostriol (Mibe, Jesalis), Vectical (Galderma), and Rolsical (Sun Pharma).[citation needed]
↑ World Health Organization (2023). The selection and use of essential medicines 2023: web annex A: World Health Organization model list of essential medicines: 23rd list (2023). Geneva: World Health Organization. hdl:10665/371090. WHO/MHP/HPS/EML/2023.02.
↑ Kircik L (August 2009). "Efficacy and safety of topical calcitriol 3 microg/g ointment, a new topical therapy for chronic plaque psoriasis". Journal of Drugs in Dermatology. 8 (8 Suppl): s9–16. PMID19702031.
↑ Kin KC, Hill D, Feldman SR (June 2016). "Calcipotriene and betamethasone dipropionate for the topical treatment of plaque psoriasis". Expert Review of Clinical Pharmacology. 9 (6): 789–797. doi:10.1080/17512433.2016.1179574. PMID27089906. S2CID38261070.
↑ Smith EL, Pincus SH, Donovan L, Holick MF (September 1988). "A novel approach for the evaluation and treatment of psoriasis. Oral or topical use of 1,25-dihydroxyvitamin D3 can be a safe and effective therapy for psoriasis". Journal of the American Academy of Dermatology. 19 (3): 516–528. doi:10.1016/S0190-9622(88)70207-8. PMID2459166.
↑ Huckins D, Felson DT, Holick M (November 1990). "Treatment of psoriatic arthritis with oral 1,25-dihydroxyvitamin D3: a pilot study". Arthritis and Rheumatism. 33 (11): 1723–1727. doi:10.1002/art.1780331117. PMID2242069.
1 2 Mazzaferro S, Goldsmith D, Larsson TE, Massy ZA, Cozzolino M (March 2014). "Vitamin D metabolites and/or analogs: which D for which patient?". Current Vascular Pharmacology. 12 (2): 339–349. doi:10.2174/15701611113119990024. PMID23713876.
↑ Levine BS, Singer FR, Bryce GF, Mallon JP, Miller ON, Coburn JW (1985). "Pharmacokinetics and biologic effects of calcitriol in normal humans". The Journal of Laboratory and Clinical Medicine. 105 (2): 239–246. ISSN0022-2143. PMID3838330.
↑ Holick MF, Schnoes HK, DeLuca HF, Suda T, Cousins RJ (July 1971). "Isolation and identification of 1,25-dihydroxycholecalciferol. A metabolite of vitamin D active in intestine". Biochemistry. 10 (14): 2799–2804. doi:10.1021/bi00790a023. PMID4326883.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.