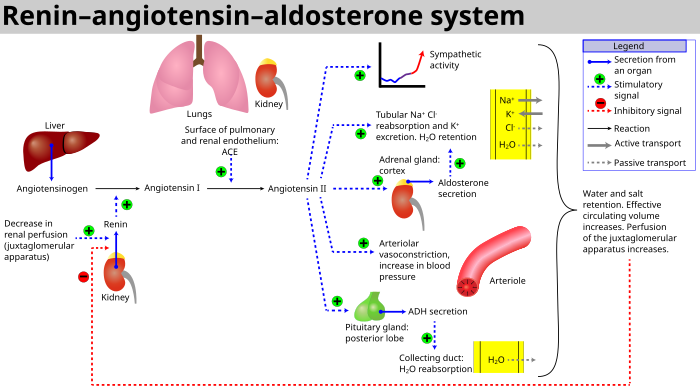
When renal blood flow is reduced, juxtaglomerular cells in the kidneys convert the precursor prorenin (already present in the blood) into renin and secrete it directly into the circulation. Plasma renin then carries out the conversion of angiotensinogen, released by the liver, to a decapeptide called angiotensin I, which has no biological function on its own.[4] Angiotensin I is subsequently converted to the active angiotensin II (an octapeptide) by the angiotensin-converting enzyme (ACE) found on the surface of vascular endothelial cells, predominantly those of the lungs.[5] Angiotensin II has a short life of about 1 to 2 minutes. Then, it is rapidly degraded into a heptapeptide called angiotensin III by angiotensinases which are present in red blood cells and vascular beds in many tissues.
Angiotensin III increases blood pressure and stimulates aldosterone secretion from the adrenal cortex; it has 100% adrenocortical stimulating activity and 40% vasopressor activity of angiotensin II.
Angiotensin IV also has adrenocortical and vasopressor activ vasoconstrictive peptide that causes blood vessels to narrow, resulting in increased blood pressure.[6] Angiotensin II also stimulates the secretion of the hormone aldosterone[6] from the adrenal cortex. Aldosterone causes the renal tubules to increase the reabsorption of sodium which in consequence causes the reabsorption of water into the blood, while at the same time causing the excretion of potassium (to maintain electrolyte balance). This increases the volume of extracellular fluid in the body, which also increases blood pressure.
If the perfusion of the juxtaglomerular apparatus in the kidney's macula densa decreases, then the juxtaglomerular cells (granular cells, modified pericytes in the glomerular capillary) release the enzymerenin.
Renin cleaves a [[Peptide#Notes on terminology005 }}</ref> which is thought to be found mainly in endothelial cells of the capillaries throughout the body, within the lungs and the epithelial cells of the kidneys. One study in 1992 found ACE in all blood vessel endothelial cells.[9]
Angiotensin I may have some minor activity, but angiotensin II is the major bio-active product. Angiotensin II has a variety of effects on the body:[citation needed]
In the kidneys, angiotensin II constricts glomerular arterioles, having a greater effect on efferent arterioles than afferent. As with most other capillary beds in the body, the constriction of afferent arterioles increases the arteriolar resistance, raising systemicarterial blood pressure and decreasing the blood flow. However, the kidneys must continue to filter enough blood despite this drop in blood flow, necessitating mechanisms to keep glomerular blood pressure up. To do this, angiotensin II constricts efferent arterioles, which forces blood to build up in the glomerulus, increasing glomerular pressure. The glomerular filtration rate (GFR) is thus maintained, and blood filtration can continue despite lowered overall kidney blood flow. Because the filtration fraction, which is the ratio of the glomerular filtration rate (GFR) to the renal plasma flow (RPF), has increased, there is less plasma fluid in the downstream peritubular capillaries. This in turn leads to a decreased hydrostatic pressure and increased oncotic pressure (due to unfiltered plasma proteins) in the peritubular capillaries. The effect of decreased hydrostatic pressure and increased oncotic pressure in the peritubular capillaries will facilitate increased reabsorption of tubular fluid.
Angiotensin II decreases medullary blood flow through the vasa recta. This decreases the washout of NaCl and urea in the kidney medullary space. Thus, higher concentrations of NaCl and urea in the medulla facilitate increased absorption of tubular fluid. Furthermore, increased reabsorption of fluid into the medulla will increase passive reabsorption of sodium along the thick ascending limb of the Loop of Henle.
Angiotensin II stimulates Na+ /H+ exchangers located on the apical membranes (faces the tubular lumen) of cells in the proximal tubule and thick ascending limb of the loop of Henle in addition to Na+ channels in the collecting ducts. This will ultimately lead to increased sodium reabsorption.
Angiotensin II stimulates the hypertrophy of renal tubule cells, leading to further sodium reabsorption.
In the adrenal cortex, angiotensin II acts to cause the release of aldosterone. Aldosterone acts on the tubules (e.g., the distal convoluted tubules and the corticalcollecting ducts) in the kidneys, causing them to reabsorb more sodium and water from the urine. This increases blood volume and, therefore, increases blood pressure. In exchange for the reabsorbing of sodium to blood, potassium is secreted into the tubules, becomes part of urine and is excreted.
Angiotensin II causes the release of anti-diuretic hormone (ADH),[6] also called vasopressin – ADH is made in the hypothalamus and released from the posterior pituitary gland. As its name suggests, it also exhibits vaso-constrictive properties, but its main course of action is to stimulate reabsorption of water in the kidneys. ADH also acts on the central nervous system to increase an individual's appetite for salt, and to stimulate the sensation of thirst.
These effects directly act together to increase blood pressure and are opposed by atrial natriuretic peptide (ANP).
Local renin–angiotensin systems
Locally expressed renin–angiotensin systems have been found in a number of tissues, including the kidneys, adrenal glands, the heart, vasculature and nervous system, and have a variety of functions, including local cardiovascular regulation, in association or independently of the systemic renin–angiotensin system, as well as non-cardiovascular functions.[10][11][12] Outside the kidneys, renin is predominantly picked up from the circulation but may be secreted locally in some tissues; its precursor prorenin is highly expressed in tissues and more than half of circulating prorenin is of extrarenal origin, but its physiological role besides serving as precursor to renin is still unclear.[13] Outside the liver, angiotensinogen is picked up from the circulation or expressed locally in some tissues; with renin they form angiotensin I, and locally expressed angiotensin-converting enzyme, chymase or other enzymes can transform it into angiotensin II.[13][14][15] This process can be intracellular or interstitial.[10]
In the adrenal glands, it is likely involved in the paracrine regulation of aldosterone secretion; in the heart and vasculature, it may be involved in remodeling or vascular tone; and in the brain, where it is largely independent of the circulatory RAS, it may be involved in local blood pressure regulation.[10][12][16] In addition, both the central and peripheral nervous systems can use angiotensin for sympathetic neurotransmission.[17] Other places of expression include the reproductive system, the skin and digestive organs. Medications aimed at the systemic system may affect the expression of those local systems, beneficially or adversely.[10]
Fetal renin–angiotensin system
In the fetus, the renin–angiotensin system is predominantly a sodium-losing system,[citation needed] as angiotensin II has little or no effect on aldosterone levels. Renin levels are high in the fetus, while angiotensin II levels are significantly lower; this is due to the limited pulmonary blood flow, preventing ACE (found predominantly in the pulmonary circulation) from having its maximum effect.[citation needed]
Clinical significance
Flowchart showing the clinical effects of RAAS activity and the sites of action of ACE inhibitors and angiotensin receptor blockers.
ACE inhibitors of angiotensin-converting enzyme inhibitors are often used to reduce the formation of the more potent angiotensin II. Captopril is an example of an ACE inhibitor. ACE cleaves a number of other peptides, and in this capacity is an important regulator of the kinin–kallikrein system, as such blocking ACE can lead to side effects.[18]
Atrial natriuretic peptide: When the atrium stretches, blood pressure is considered to be increased and sodium is excreted to lower blood pressure.
Bainbridge reflex: In response to stretching of the right atrium wall, heart rate increases, lowering venous blood pressure.
Baroreflex: When the stretch receptors in the aortic arch and carotid sinus increase, the blood pressure is considered to be elevated and the heart rate decreases to lower blood pressure.
Antidiuretic hormone: The hypothalamus detects the extracellular fluid hyperosmolality and the posterior pituitary gland secretes antidiuretic hormone to increase water reabsorption in the collecting duct.
↑ Rogerson FM, Chai SY, Schlawe I, Murray WK, Marley PD, Mendelsohn FA (July 1992). "Presence of angiotensin converting enzyme in the adventitia of large blood vessels". J. Hypertens. 10 (7): 615–620. doi:10.1097/00004872-199207000-00003. PMID1321187. S2CID25785488.
↑ Kumar R, Singh VP, Baker KM (March 2008). "The intracellular renin-angiotensin system: implications in cardiovascular remodeling". Current Opinion in Nephrology and Hypertension. 17 (2): 168–173. doi:10.1097/MNH.0b013e3282f521a8. PMID18277150. S2CID39068591.
↑ McKinley MJ, Albiston AL, Allen AM, Mathai ML, May CN, McAllen RM, etal. (June 2003). "The brain renin-angiotensin system: location and physiological roles". The International Journal of Biochemistry & Cell Biology. 35 (6): 901–918. doi:10.1016/S1357-2725(02)00306-0. PMID12676175.
↑ Patil J, Heiniger E, Schaffner T, Mühlemann O, Imboden H (April 2008). "Angiotensinergic neurons in sympathetic coeliac ganglia innervating rat and human mesenteric resistance blood vessels". Regulatory Peptides. 147 (1–3): 82–87. doi:10.1016/j.regpep.2008.01.006. PMID18308407. S2CID23123825.
↑ Richter WF, Whitby BR, Chou RC (1996). "Distribution of remikiren, a potent orally active inhibitor of human renin, in laboratory animals". Xenobiotica. 26 (3): 243–254. doi:10.3109/00498259609046705. PMID8730917.
↑ Tissot AC, Maurer P, Nussberger J, Sabat R, Pfister T, Ignatenko S, etal. (March 2008). "Effect of immunisation against angiotensin II with CYT006-AngQb on ambulatory blood pressure: a double-blind, randomised, placebo-controlled phase IIa study". Lancet. 371 (9615): 821–827. doi:10.1016/S0140-6736(08)60381-5. PMID18328929. S2CID15175992.
Banic A, Sigurdsson GH, Wheatley AM (1993). "Influence of age on the cardiovascular response during graded haemorrhage in anaesthetized rats". Res Exp Med (Berl). 193 (5): 315–321. doi:10.1007/BF02576239. PMID8278677. S2CID37700794.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.