Mechanism of action
Progesterone is a progestogen, or an agonist of the nuclear progesterone receptors (PRs), the PR-A, PR-B, and PR-C. [1] In one study, progesterone showed EC50 values of 7.7 nM for the human PR-A and 8.0 nM for the human PR-B. [5] In addition to the PRs, progesterone is an agonist of the membrane progesterone receptors (mPRs), including the mPRα, mPRβ, mPRγ, mPRδ, and mPRϵ. [6] [7] It is also a potent antimineralocorticoid (antagonist of the mineralocorticoid receptor (MR)), [8] [9] as well as a very weak glucocorticoid (agonist of the glucocorticoid receptor). [10] [11] Progesterone does not interact significantly with the androgen receptor (AR) or with the estrogen receptor (ER). [1] In addition to its activity as a steroid hormone, progesterone is a neurosteroid. [12] Specifically, it is an antagonist of the sigma σ1 receptor, [13] [14] a negative allosteric modulator of nicotinic acetylcholine receptors, [12] and, via its active metabolites allopregnanolone and pregnanolone, a potent positive allosteric modulator of the GABAA receptor, the major signaling receptor of the inhibitory neurotransmitter γ-aminobutyric acid (GABA). [15]
| Compound | PR | AR | ER | GR | MR | SHBG | CBG |
|---|---|---|---|---|---|---|---|
| Progesterone | 50 | 0 | 0 | 10 | 100 | 0 | 36 |
| Notes: Values are percentages (%). Reference ligands (100%) were promegestone for the PR , metribolone for the AR , E2 for the ER , DEXA for the GR , aldosterone for the MR , DHT for SHBG , and cortisol for CBG . Sources: [1] | |||||||
| Compound | Form | Dose for specific uses (mg) [lower-alpha 3] | DOA [lower-alpha 4] | |||
|---|---|---|---|---|---|---|
| TFD [lower-alpha 5] | POICD [lower-alpha 6] | CICD [lower-alpha 7] | ||||
| Algestone acetophenide | Oil soln. | - | – | 75–150 | 14–32 d | |
| Gestonorone caproate | Oil soln. | 25–50 | – | – | 8–13 d | |
| Hydroxyprogest. acetate [lower-alpha 8] | Aq. susp. | 350 | – | – | 9–16 d | |
| Hydroxyprogest. caproate | Oil soln. | 250–500 [lower-alpha 9] | – | 250–500 | 5–21 d | |
| Medroxyprog. acetate | Aq. susp. | 50–100 | 150 | 25 | 14–50+ d | |
| Megestrol acetate | Aq. susp. | - | – | 25 | >14 d | |
| Norethisterone enanthate | Oil soln. | 100–200 | 200 | 50 | 11–52 d | |
| Progesterone | Oil soln. | 200 [lower-alpha 9] | – | – | 2–6 d | |
| Aq. soln. | ? | – | – | 1–2 d | ||
| Aq. susp. | 50–200 | – | – | 7–14 d | ||
Notes and sources:
| ||||||
Antimineralocorticoid activity
Progesterone is a potent antimineralocorticoid. [8] [9] [35] It has 1000% of the affinity of aldosterone, the major endogenous agonist, for the human MR, and 100% of the affinity of aldosterone for the rat MR. [36] [1] [8] Progesterone produces antimineralocorticoid effects such as natriuresis (excretion of sodium in the urine) at normal physiological concentrations. [9] A 200 mg dose of oral progesterone is considered to be approximately equivalent in antimineralocorticoid effect to a 25 to 50 mg dose of the potent antimineralocorticoid spironolactone, which itself is a derivative of progesterone. [37] Doses of progesterone of 50 to 200 mg by intramuscular injection, which are similar to progesterone exposure in the third trimester of pregnancy, have also been reported to produce antimineralocorticoid-like effects. [35] The antimineralocorticoid effects of progesterone underlie its ability to lower blood pressure and reduce water and salt retention and its potential application in the treatment of hypertension. [38] [1] [39] [35] An active metabolite of progesterone, 11-deoxycorticosterone (21-hydroxyprogesterone), is a precursor of aldosterone and has strong mineralocorticoid activity (i.e., is a strong agonist of the MR). [37] However, it is formed in relatively small amounts, and any such effects produced by it are usually outweighed by the antimineralocorticoid activity of progesterone. [37] Progesterone may be a relatively weak antimineralocorticoid in vivo. [40]
Glucocorticoid activity
Progesterone is a partial agonist of the glucocorticoid receptor (GR). [1] [10] [11] [41] [42] It has about 35% of the affinity of dexamethasone, a corticosteroid, for the human GR, and about 3 to 11% of the affinity of dexamethasone for the rat GR. [36] However, progesterone appears to show weak or no glucocorticoid activity and no antiglucocorticoid activity in vitro and in animals. [42] Nonetheless, progesterone has been found to upregulate the thrombin receptor in vascular smooth muscle cells in vitro, a glucocorticoid effect, and this could have clinical relevance in relation to risk of blood clots. [1] [43]
| Steroid | Class | TR (↑)a | GR (%)b |
|---|---|---|---|
| Dexamethasone | Corticosteroid | ++ | 100 |
| Ethinylestradiol | Estrogen | – | 0 |
| Etonogestrel | Progestin | + | 14 |
| Gestodene | Progestin | + | 27 |
| Levonorgestrel | Progestin | – | 1 |
| Medroxyprogesterone acetate | Progestin | + | 29 |
| Norethisterone | Progestin | – | 0 |
| Norgestimate | Progestin | – | 1 |
| Progesterone | Progestogen | + | 10 |
| Footnotes:a = Thrombin receptor (TR) upregulation (↑) in vascular smooth muscle cells (VSMCs). b = RBA (%) for the glucocorticoid receptor (GR). Strength: – = No effect. + = Pronounced effect. ++ = Strong effect. Sources: [44] | |||
Androgenic and antiandrogenic activity
The binding and activity of progesterone at the androgen receptor (AR), the biological target of androgens like testosterone and dihydrotestosterone (DHT) in the body, is controversial. [45] Some studies have found progesterone to bind to the AR, with agonistic and antagonistic activity exerted, whereas other studies have found very low or no affinity for the AR at all. [45] In animal studies, no androgenic effects have been observed, but weak antiandrogenic effects have been reported. [45] The weak antiandrogenic activity has been attributed not to antagonism of the AR by progesterone, but rather to its weak 5α-reductase inhibition and consequent inhibition of the conversion of testosterone into the more potent DHT. [45] There is no clinical evidence of AR-mediated androgenic or antiandrogenic activity with progesterone. [45] Progesterone has not been associated with any classical androgenic effects in clinical studies in women, including no changes in the blood lipid profile or sex hormone-binding globulin levels, acne, oily skin, hirsutism, or voice deepening, nor with virilization of female fetuses. [46] [47] [48] [49] [50] As such, the scientific consensus is that progesterone is clinically neither androgenic nor antiandrogenic. [1] [51] [52] This is in contrast to many progestins, such as 19-nortestosterone derivatives (e.g., norethisterone, levonorgestrel, dienogest) and 17α-hydroxyprogesterone derivatives (e.g., cyproterone acetate, medroxyprogesterone acetate), which do bind to the AR and have been associated with significant androgenic or antiandrogenic effects depending on the progestin in question. [1] [52] Due to its lack of androgenic and antiandrogenic activity, and hence lack of masculinizing and feminizing effects, progesterone is one of the few progestogens that is suitable for use during pregnancy in women at risk for preterm birth or recurrent miscarriage. [53] [54]
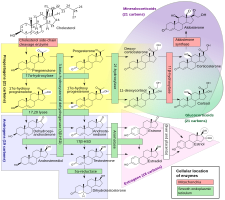
Although progesterone does not have significant AR-mediated androgenic or antiandrogenic activity, it is a precursor and intermediate, albeit distant, in the biosynthesis of androgens from cholesterol. [55] [56] For this reason, there has been some speculation that exogenous progesterone could be transformed into androgens by certain tissues that express the requisite enzymes. [56] [57] Progesterone is converted by 17α-hydroxylase into 17α-hydroxyprogesterone; 17α-hydroxyprogesterone is converted by 17,20-lyase into androstenedione; and androstenedione is converted by 17β-hydroxysteroid dehydrogenases into testosterone. [55] CYP17A1, the cytochrome P450 gene that encodes 17α-hydroxylase and 17,20-lyase, is expressed mainly in the gonads (ovaries and testes) and the adrenal glands. [58] However, while it is theoretically possible that progesterone could be transformed in the body into androgens, no androgenic effects have been observed in animal studies. [45] In addition, clinical studies, in which women were treated with 100 to 300 mg/day oral progesterone, have found no or only a small increase in levels of 17α-hydroxyprogesterone, and no change in androgen levels, including of dehydroepiandrosterone, androstenedione, and testosterone. [50] [59] [46] In these studies, levels of estradiol and cortisol, which progesterone is also a precursor of, did not change either, although levels of 11-deoxycorticosterone increased significantly. [59] [46] Levels of androgens, like testosterone and dihydrotestosterone (DHT), also do not increase going from the follicular phase to the luteal phase of the menstrual cycle in premenopausal women (progesterone levels being high in the luteal phase). [60]
5α-Reductase inhibition
Progesterone is a substrate for 5α-reductase, and has been found to act as a competitive inhibitor of this enzyme in vitro in a variety of studies. [1] In one study, it showed IC50 values of 1,375 nM and 88 nM (in the presence of 50 nM androstenedione as the substrate) for 5α-reductase types 1 and 2, respectively. [61] 5α-Reductase is highly expressed in skin, hair follicles, and prostate gland, and is responsible for the transformation of testosterone into the several-fold more potent androgen DHT in such tissues. [62] [63] As such, it has been suggested that progesterone might possess some antiandrogenic effect via acting as a 5α-reductase inhibitor. [1] However, inhibition of 5α-reductase by progesterone is described as a weak effect that has only been demonstrated in vitro and at supraphysiological concentrations. [64] [65] In accordance, physiological levels of circulating progesterone have not been found to importantly influence circulating DHT concentrations. [60] [66]
Congenital 5α-reductase 2 deficiency is a rare intersex condition which is associated with ambiguous genitalia in male fetuses due to a deficiency in DHT production during genital differentiation. [63] Experimental prenatal exposure to established 5α-reductase inhibitors like finasteride has been found to produce similar feminized genital defects in male animals including rodents and monkeys. [67] In contrast, exogenous administration of progesterone to pregnant rodents and monkeys has resulted in minimal abnormality in either male or female pups. [68] [69] [70] [71] In addition, endogenous progesterone levels naturally increase to extremely high concentrations during pregnancy, yet genital defects do not occur. [72] In accordance, while total concentrations of progesterone in pregnant women at term are around 150 ng/mL (~500 nM), free or unbound and hence bioactive concentrations of progesterone are only about 3 ng/mL (~10 nM) due to the high plasma protein binding of progesterone, and these concentrations are still well below the aforementioned IC50 values for inhibition of 5α-reductase types 1 and 2. [73] [74] As with endogenous progesterone during pregnancy, exogenous supplemental progesterone during pregnancy has been found not to increase the risk of hypospadias in male infants. [75]
Although systemic progesterone does not appear to be an effective 5α-reductase inhibitor, topical progesterone may produce potent inhibition of 5α-reductase in the skin due to the very high local concentrations that occur. [76] [77] A study found that topical progesterone applied to the pubic area in men inhibited 5α-reductase in the skin in this region by 75%. [77] [78] In addition to inhibition of 5α-reductase, progesterone is metabolized by 5α-reductase into 5α-dihydroprogesterone (5α-DHP), a compound reported to have some antagonistic activity at the AR. [78] [79] However, this compound appears to have no systemic antiandrogenic activity. [80] In spite of its apparent 5α-reductase inhibition, the effectiveness of topical progesterone in the treatment of pattern hair loss has been poor. [79] [81] [82]
Other activity
Certain progestins have been found to stimulate the proliferation of MCF-7 breast cancer cells in vitro , an action that is independent of the classical PRs and is instead mediated via the progesterone receptor membrane component-1 (PGRMC1). [83] Progesterone, nomegestrol acetate, and chlormadinone acetate act neutrally and do not stimulate proliferation, whereas norethisterone, desogestrel, levonorgestrel, and drospirenone strongly stimulate proliferation and medroxyprogesterone acetate, dienogest, and dydrogesterone weakly stimulate proliferation. [83] [84] As such, progesterone differs from some but not all progestins in the activity mediating this PGRMC1-dependent effect. [83] It is unclear if these findings may explain the different risks of breast cancer observed with progesterone, dydrogesterone, and other progestins such as medroxyprogesterone acetate and norethisterone in clinical studies. [85]