
The foot is an anatomical structure found in many vertebrates. It is the terminal portion of a limb which bears weight and allows locomotion. In many animals with feet, the foot is a separate organ at the terminal part of the leg made up of one or more segments or bones, generally including claws and or nails.

The human leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. The thigh is between the hip and knee, while the calf (rear) and shin (front) are between the knee and foot.

The heel is the prominence at the posterior end of the foot. It is based on the projection of one bone, the calcaneus or heel bone, behind the articulation of the bones of the lower leg.

In human anatomy, the fibularis longus is a superficial muscle in the lateral compartment of the leg. It acts to tilt the sole of the foot away from the midline of the body (eversion) and to extend the foot downward away from the body at the ankle.
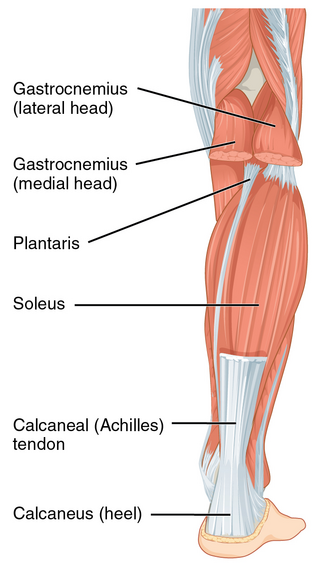
The Achilles tendon or heel cord, also known as the calcaneal tendon, is a tendon at the back of the lower leg, and is the thickest in the human body. It serves to attach the plantaris, gastrocnemius (calf) and soleus muscles to the calcaneus (heel) bone. These muscles, acting via the tendon, cause plantar flexion of the foot at the ankle joint, and flexion at the knee.
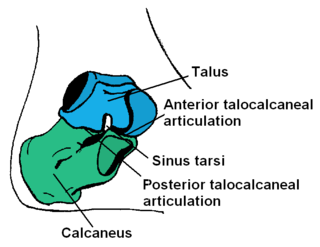
In humans and many other primates, the calcaneus or heel bone is a bone of the tarsus of the foot which constitutes the heel. In some other animals, it is the point of the hock.

Pes cavus, also known as high arch, is a human foot type in which the sole of the foot is distinctly hollow when bearing weight. That is, there is a fixed plantar flexion of the foot. A high arch is the opposite of a flat foot and is somewhat less common.

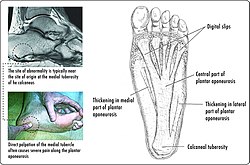
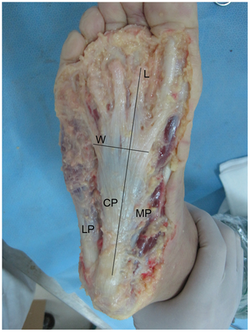
Plantar fasciitis or plantar heel pain is a disorder of the plantar fascia, which is the connective tissue which supports the arch of the foot. It results in pain in the heel and bottom of the foot that is usually most severe with the first steps of the day or following a period of rest. Pain is also frequently brought on by bending the foot and toes up towards the shin. The pain typically comes on gradually, and it affects both feet in about one-third of cases.

Flat feet is a postural deformity in which the arches of the foot collapse, with the entire sole of the foot coming into complete or near-complete contact with the ground. Sometimes children are born with flat feet (congenital).
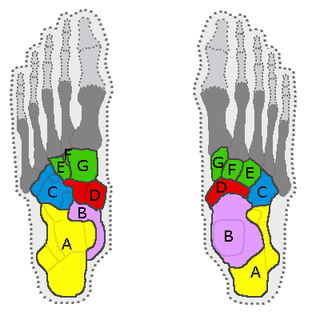
In the human body, the tarsus is a cluster of seven articulating bones in each foot situated between the lower end of the tibia and the fibula of the lower leg and the metatarsus. It is made up of the midfoot and hindfoot.

In human anatomy, the dorsal interossei of the foot are four muscles situated between the metatarsal bones.
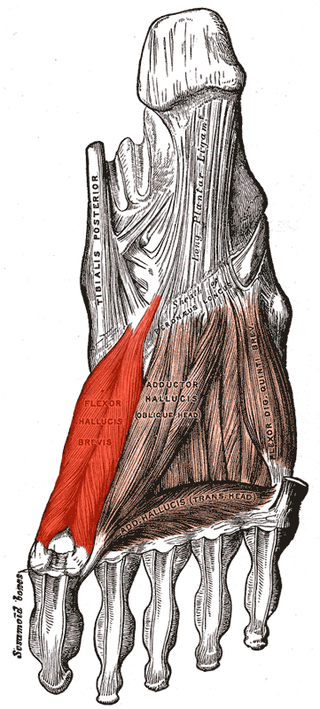
Flexor hallucis brevis muscle is a muscle of the foot that flexes the big toe.

A calcaneal spur is a bony outgrowth from the calcaneal tuberosity. Calcaneal spurs are typically detected by x-ray examination. It is a form of exostosis.

The sole is the bottom of the foot.

The arches of the foot, formed by the tarsal and metatarsal bones, strengthened by ligaments and tendons, allow the foot to support the weight of the body in the erect posture with the least weight.

The fifth metatarsal bone is a long bone in the foot, and is palpable along the distal outer edges of the feet. It is the second smallest of the five metatarsal bones. The fifth metatarsal is analogous to the fifth metacarpal bone in the hand.
The Ponseti method is a manipulative technique that corrects congenital clubfoot without invasive surgery. It was developed by Ignacio V. Ponseti of the University of Iowa Hospitals and Clinics, USA in the 1950s, and was repopularized in 2000 by John Herzenberg in the US and Europe and in Africa by NHS surgeon Steve Mannion. It is a standard treatment for clubfoot.
In the human foot, the plantar or volar plates are fibrocartilaginous structures found in the metatarsophalangeal (MTP) and interphalangeal (IP) joints. The anatomy and composition of the plantar plates are similar to the palmar plates in the metacarpophalangeal (MCP) and interphalangeal joints in the hand; the proximal origin is thin but the distal insertion is stout. Due to the weight-bearing nature of the human foot, the plantar plates are exposed to extension forces not present in the human hand.

Locomotor effects of shoes are the way in which the physical characteristics or components of shoes influence the locomotion neuromechanics of a person. Depending on the characteristics of the shoes, the effects are various, ranging from alteration in balance and posture, muscle activity of different muscles as measured by electromyography (EMG), and the impact force. There are many different types of shoes that exist, such as running, walking, loafers, high heels, sandals, slippers, work boots, dress shoes, and many more. However, a typical shoe will be composed of an insole, midsole, outsole, and heels, if any. In an unshod condition, where one is without any shoes, the locomotor effects are primarily observed in the heel strike patterns and resulting impact forces generated on the ground.

A plantar fascial rupture, is a painful tear in the plantar fascia. The plantar fascia is a connective tissue that spans across the bottom of the foot. The condition plantar fasciitis may increase the likelihood of rupture. A plantar fascial rupture may be mistaken for plantar fasciitis or even a calcaneal fracture. To allow for proper diagnosis, an MRI is often needed.



{kind=link}