Cimetidine was the prototypical histamine H2 receptor antagonist from which later drugs were developed. Cimetidine was the culmination of a project at Smith, Kline & French (SK&F; now GlaxoSmithKline) by James W. Black, C. Robin Ganellin, and others to develop a histamine receptor antagonist that would suppress stomach acid secretion.
In 1964, it was known that histamine stimulated the secretion of stomach acid, and also that traditional antihistamines had no effect on acid production. From these facts the SK&F scientists postulated the existence of two different types of histamine receptors. They designated the one acted upon by the traditional antihistamines as H1, and the one acted upon by histamine to stimulate the secretion of stomach acid as H2.
The SK&F team used a classical design process starting from the structure of histamine. Hundreds of modified compounds were synthesised in an effort to develop a model of the then-unknown H2 receptor. The first breakthrough was Nα-guanylhistamine, a partial H2receptor antagonist. From this lead, the receptor model was further refined, which eventually led to the development of burimamide, a specific competitive antagonist at the H2 receptor. Burimamide is 100 times more potent than Nα-guanylhistamine, proving its efficacy on the H2 receptor.
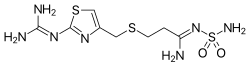
The potency of burimamide was still too low for oral administration. And efforts on further improvement of the structure, based on the structure modification in the stomach due to the acid dissociation constant of the compound, led to the development of metiamide. Metiamide was an effective agent; however, it was associated with unacceptable nephrotoxicity and agranulocytosis. It was proposed that the toxicity arose from the thiourea group, and similar guanidine analogues were investigated until the discovery of cimetidine, which would become the first clinically successful H2 antagonist.
Ranitidine (common brand name Zantac) was developed by Glaxo (also now GlaxoSmithKline), in an effort to match the success of Smith, Kline & French with cimetidine. Ranitidine was also the result of a rational drug design process utilising the by-then-fairly-refined model of the histamine H2 receptor and quantitative structure-activity relationships (QSAR). Glaxo refined the model further by replacing the imidazole-ring of cimetidine with a furan-ring with a nitrogen-containing substituent, and in doing so developed ranitidine, which was found to have a much better tolerability profile (i.e. fewer adverse drug reactions), longer-lasting action, and ten times the activity of cimetidine.
Ranitidine was introduced in 1981 and was the world's biggest-selling prescription drug by 1988. The H2 receptor antagonists have since largely been superseded by the even more effective proton pump inhibitors (PPIs), with omeprazole becoming the biggest-selling drug for many years.
Pharmacology
The H2 antagonists are competitive antagonists of histamine at the parietal cell's H2 receptor. They suppress the normal secretion of acid by parietal cells and the meal-stimulated secretion of acid. They accomplish this by two mechanisms: Histamine released by enterochromaffin-like cells (ECL) in the stomach is blocked from binding on parietal cell H2 receptors, which stimulate acid secretion; therefore, other substances that promote acid secretion (such as gastrin and acetylcholine) have a reduced effect on parietal cells when the H2 receptors are blocked.
Prevention of stress ulcer (a specific indication of ranitidine)
Prevention of aspiration pneumonitis during surgery. Oral H2 antagonists reduce gastric acidity and volume and have shown to reduce the frequency of aspiration pneumonitis; however, this aspiration benefit has not been shown with IV H2antagonists.[8]
People who suffer from infrequent heartburn may take either antacids or H2 receptor antagonists for treatment. The H2 antagonists offer several advantages over antacids, including longer duration of action (6–10 hours vs 1–2 hours for antacids), greater efficacy, and ability to be used prophylactically before meals to reduce the chance of heartburn occurring. Proton pump inhibitors, however, are the preferred treatment for erosive esophagitis since they have been shown to promote healing better than H2antagonists.[9]
Adverse effects
H2 antagonists are generally well tolerated, with the exception of cimetidine, which more commonly elicits the following adverse drug reactions (ADRs) than other H2 antagonists:
Infrequent ADRs include hypotension. Rare ADRs include headache, tiredness, dizziness, confusion, diarrhea, constipation, and rash.[7] In addition, gynecomastia occurred in 0.1–0.5% of men treated for non-hypersecretory conditions with cimetidine for 1 month or longer and in about 2% of men treated for pathologic hypersecretory conditions; in even fewer men, cimetidine may also cause loss of libido, and impotence, all of which are reversible upon discontinuation.[10]
A 31-study review found that the overall risk of pneumonia is about 1 in 4 higher among H2 antagonist users.[11]
Famotidine has been associated with agranulocytosis, the destruction of white blood cells.[13]
Research
Bladder diseases
Histamine can cause bladder inflammation and contribute to the symptoms of such bladder diseases as cystitis (inflammation of the bladder) or painful bladder disease. Histamine binds to H2 receptors in the bladder smooth muscle, leading to relaxation[contradictory] of the bladder muscle and promotion of urine storage. Histamine does not seem to have a direct role in the development of bladder diseases, but it can contribute to bladder inflammation and associated symptoms.
H2 receptors in the bladder play a role in regulating bladder contraction.
H2 receptor antagonists have been shown to reduce bladder contractions and improve bladder function in animal studies.[14][15][16] Blocking the activation of H2 receptors in the bladder leads to decreased bladder contractions and improved urine storage. While H2 receptor antagonists may have a potential role in managing bladder conditions such as overactive bladder, they are not typically used in treating cystitis or painful bladder disease, and their mechanism of action in bladder diseases is still not fully understood. There is limited research that histamine H2 receptor antagonists can potentially alleviate symptoms of cystitis[17][18] or painful bladder disease.[19][20][21]
Drug interactions
Skeletal formula of famotidine. Unlike cimetidine, famotidine has no significant interactions with other drugs.
The more recently developed H2receptor antagonists are less likely to alter CYP metabolism. Ranitidine is not as potent a CYP inhibitor as cimetidine, although it still shares several of the latter's interactions (such as with warfarin, theophylline, phenytoin, metoprolol, and midazolam).[23]Famotidine has negligible effect on the CYP system, and appears to have no significant interactions.[22]
↑Eriksson S, Långström G, Rikner L, Carlsson R, Naesdal J (1995). "Omeprazole and H2-receptor antagonists in the acute treatment of duodenal ulcer, gastric ulcer and reflux oesophagitis: a meta-analysis". Eur J Gastroenterol Hepatol. 7 (5): 467–75. PMID7614110.. A correction was published in European Journal of Gastroenterology & Hepatology 1996;8:192.
↑Gasbarrini G, Gentiloni N, Febbraro S, Gasbarrini A, Di Campli C, Cesana M, Miglio F, Miglioli M, Ghinelli F, d'Ambrosi A, Amoroso P, Pacini F, Salvadori G (1997). "Acute liver injury related to the use of niperotidine". Journal of Hepatology. 27 (3): 583–586. doi:10.1016/s0168-8278(97)80365-0. PMID9314138.
↑Miller RD, Eriksson L, Fleisher LA, Wiener-Kronish JP (25 November 2014). Miller's Anesthesia Airway management in the Adult (8thed.). Elsevier. pp.1647–1681.
↑Katz PO, Gerson LB, Vela MF (March 2013). "Guidelines for the Diagnosis and Management of Gastroesophageal Reflux Disease". American Journal of Gastroenterology. 108 (3): 308–328. doi:10.1038/ajg.2012.444. PMID23419381.
↑Meng R, Chen LR, Zhang ML, Cai WK, Yin SJ, Fan YX, Zhou T, Huang YH, He GH (2023). "Effectiveness and Safety of Histamine H2 Receptor Antagonists: An Umbrella Review of Meta-Analyses". The Journal of Clinical Pharmacology. 63 (1): 7–20. doi:10.1002/jcph.2147. PMID36039014. S2CID251931004.
↑Marcus EL, Clarfield AM, Kleinman Y, Bits H, Darmon D, Da'as N (February 2002). "Agranulocytosis associated with initiation of famotidine therapy". Annals of Pharmacotherapy. 36 (2): 267–271. doi:10.1345/aph.1A045. PMID11847947.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.