Anemia is a decrease in the total amount of red blood cells (RBCs) or hemoglobin in the blood, or a lowered ability of the blood to carry oxygen. When anemia comes on slowly, the symptoms are often vague and may include feeling tired, weakness, shortness of breath, and a poor ability to exercise. When the anemia comes on quickly, symptoms may include confusion, feeling like one is going to pass out, loss of consciousness, and increased thirst. Anemia must be significant before a person becomes noticeably pale. Additional symptoms may occur depending on the underlying cause.
Fever, also known as pyrexia and febrile response, is defined as having a temperature above the normal range due to an increase in the body's temperature set point. There is not a single agreed-upon upper limit for normal temperature with sources using values between 37.5 and 38.3 °C. The increase in set point triggers increased muscle contractions and causes a feeling of cold. This results in greater heat production and efforts to conserve heat. When the set point temperature returns to normal, a person feels hot, becomes flushed, and may begin to sweat. Rarely a fever may trigger a febrile seizure. This is more common in young children. Fevers do not typically go higher than 41 to 42 °C.
Vomiting is the involuntary, forceful expulsion of the contents of one's stomach through the mouth and sometimes the nose.
Escherichia coli O157:H7 is a serotype of the bacterial species Escherichia coli and is one of the Shiga toxin–producing types of E. coli. It is a cause of disease, typically foodborne illness, through consumption of contaminated and raw food, including raw milk and undercooked ground beef. Infection with this type of pathogenic bacteria may lead to hemorrhagic diarrhea, and to kidney failure; these have been reported to cause the deaths of children younger than five years of age, of elderly patients, and of patients whose immune systems are otherwise compromised.
Shigella is a genus of Gram-negative, facultative aerobic, non-spore-forming, nonmotile, rod-shaped bacteria genetically closely related to E. coli. The genus is named after Kiyoshi Shiga, who first discovered it in 1897.
Salmonella is a genus of rod-shaped (bacillus) Gram-negative bacteria of the family Enterobacteriaceae. The two species of Salmonella are Salmonella enterica and Salmonella bongori. S. enterica is the type species and is further divided into six subspecies that include over 2,600 serotypes. Salmonella was named after Daniel Elmer Salmon (1850–1914), an American veterinary surgeon.
In medicine, dialysis is the process of removing excess water, solutes, and toxins from the blood in people whose kidneys can no longer perform these functions naturally. This is referred to as renal replacement therapy.
Plasmapheresis is the removal, treatment, and return or exchange of blood plasma or components thereof from and to the blood circulation. It is thus an extracorporeal therapy.
A syndrome is a set of medical signs and symptoms and collection of diseases which are not correlated with each other and often associated with a particular disease or disorder. The word derives from the Greek σύνδρομον, meaning "concurrence". In some instances, a syndrome is so closely linked with a pathogenesis or cause that the words syndrome, disease, and disorder end up being used interchangeably for them. This is especially true of inherited syndromes. For example, Down syndrome, Wolf–Hirschhorn syndrome, and Andersen syndrome are disorders with known pathogeneses, so each is more than just a set of signs and symptoms, despite the syndrome nomenclature. In other instances, a syndrome is not specific to only one disease. For example, toxic shock syndrome can be caused by various toxins; premotor syndrome can be caused by various brain lesions; and premenstrual syndrome is not a disease but simply a set of symptoms.
Signs and symptoms
After eating contaminated food, the first symptoms of infection can emerge anywhere from 1 to 10 days later, but usually after 3 to 4 days.[8] These early symptoms can include diarrhea (which is often bloody), stomach cramps, mild fever,[9] or vomiting that results in dehydration and reduced urine.[8] HUS typically develops about 5–10 days after the first symptoms, but can take up to 3 weeks to manifest, and occurs at a time when the diarrhea is improving.[9] Related symptoms and signs include lethargy, decreased urine output, blood in the urine, kidney failure, low platelets, (which are needed for blood clotting), and destruction of red blood cells (microangiopathic hemolytic anemia). High blood pressure, jaundice (a yellow tinge in skin and the whites of the eyes), seizures, and bleeding into the skin can also occur.[9] In some cases, there are prominent neurologic changes.[10][11][12]
Oliguria or hypouresis is the low output of urine specifically more than 80 ml/day but less than 400ml/day. The decreased output of urine may be a sign of dehydration, kidney failure, hypovolemic shock, HHNS hyperosmolar Hyperglycemic Nonketotic Syndrome, multiple organ dysfunction syndrome, urinary obstruction/urinary retention, DKA, pre-eclampsia, and urinary tract infections, among other conditions.
Hematuria is the presence of red blood cells in the urine. Visible hematuria, also known as gross hematuria, causes visible red or brown discoloration of the urine. Microscopic hematuria is invisible to the naked eye and is often found by urinalysis or urine dipstick; it is said to be chronic or persistent if 5 or more red blood cells (RBCs) per high-power field can be seen in 3 of 3 consecutive centrifuged specimens obtained at least 1 week apart. Any part of the kidneys or urinary tract can leak blood into the urine. The causes of hematuria are broad, ranging from urinary tract infection to kidney stones to bladder cancer.
Kidney failure, also known as end-stage kidney disease, is a medical condition in which the kidneys are functioning at less than 15% of normal. Kidney failure is classified as either acute kidney failure, which develops rapidly and may resolve; and chronic kidney failure, which develops slowly. Symptoms may include leg swelling, feeling tired, vomiting, loss of appetite, and confusion. Complications of acute and chronic failure include uremia, high blood potassium, and volume overload. Complications of chronic failure also include heart disease, high blood pressure, and anemia.
People with HUS commonly exhibit the symptoms of thrombotic microangiopathy (TMA), which can include abdominal pain,[13] low platelet count,[14] elevated lactate dehydrogenase LDH, a chemical released from damaged cells, and which is therefore a marker of cellular damage)[15] decreased haptoglobin (indicative of the breakdown of red blood cells)[15] anemia (low red blood cell count), schistocytes (damaged red blood cells),[14][15] elevated creatinine (a protein waste product generated by muscle metabolism and eliminated renally,[16] proteinuria (indicative of kidney injury),[17] confusion,[13] fatigue,[18]swelling,[19] nausea/vomiting,[20] and diarrhea.[21] Additionally, patients with aHUS typically present with an abrupt onset of systemic signs and symptoms such as acute kidney failure,[14]hypertension (high blood pressure),[18] myocardial infarction (heart attack),[22] stroke,[13] lung complications,[22]pancreatitis (inflammation of the pancreas),[20] liver necrosis (death of liver cells or tissue),[14][18]encephalopathy (brain dysfunction),[18] seizure,[23] and coma.[24] Failure of neurologic, cardiac, renal, and gastrointestinal (GI) organs, as well as death, can occur unpredictably at any time, either very quickly or following prolonged symptomatic or asymptomatic disease progression.[5][6][14][17][25]
Thrombotic microangiopathy (TMA) is a pathology that results in thrombosis in capillaries and arterioles, due to an endothelial injury. It may be seen in association with thrombocytopenia, anemia, purpura and renal failure.
Lactate dehydrogenase (LDH or LD) is an enzyme found in nearly all living cells (animals, plants, and prokaryotes). LDH catalyzes the conversion of lactate to pyruvate and back, as it converts NAD+ to NADH and back. A dehydrogenase is an enzyme that transfers a hydride from one molecule to another.
Edema, also spelled oedema or œdema, is an abnormal accumulation of fluid in the interstitium, located beneath the skin and in the cavities of the body, which can cause severe pain. Clinically, hyperaldosteronism, edema manifests as swelling. The amount of interstitial fluid is determined by the balance of fluid homeostasis and the increased secretion of fluid into the interstitium. The word is from Greek οἴδημα oídēma meaning "swelling". The condition is also known as dropsy.
Shiga toxins are a family of related toxins with two major groups, Stx1 and Stx2, expressed by genes considered to be part of the genome of lambdoid prophages. The toxins are named after Kiyoshi Shiga, who first described the bacterial origin of dysentery caused by Shigella dysenteriae. Shiga-like toxin (SLT) is a historical term for similar or identical toxins produced by Escherichia coli. The most common sources for Shiga toxin are the bacteria S. dysenteriae and some serotypes of Escherichia coli (STEC), which includes serotypes O157:H7, and O104:H4.
A serotype or serovar is a distinct variation within a species of bacteria or virus or among immune cells of different individuals. These microorganisms, viruses, or cells are classified together based on their cell surface antigens, allowing the epidemiologic classification of organisms to the subspecies level. A group of serovars with common antigens is called a serogroup or sometimes serocomplex.
Atypical HUS (aHUS) represents 5–10% of HUS cases[5] and is largely due to one or several genetic mutations that cause chronic, uncontrolled, and excessive activation of complement.[5] This results in platelet activation endothelial cell damage, and white blood cell activation, leading to systemic TMA, which manifests as decreased platelet count, hemolysis (breakdown of red blood cells), damage to multiple organs, and ultimately death.[6][17][27] Early signs of systemic complement-mediated TMA include thrombocytopenia (platelet count below 150,000 or a decrease from baseline of at least 25%)[15] and evidence of microangiopathic hemolysis, which is characterized by elevated LDH levels, decreased haptoglobin, decreased hemoglobin (the oxygen-containing component of blood), and/or the presence of schistocytes.[6][28][15] Despite the use of supportive care, an estimated 33–40% of patients will die or have end-stage renal disease (ESRD) with the first clinical manifestation of aHUS,[21][22] and 65% of patients will die, require dialysis, or have permanent renal damage within the first year after diagnosis despite plasma exchange or plasma infusion (PE/PI) therapy.[21] Patients who survive the presenting signs and symptoms of aHUS endure a chronic thrombotic and inflammatory state, which puts them at lifelong elevated risk of sudden blood clotting, kidney failure, other severe complications and premature death.[28][19]
Historically, treatment options for aHUS were limited to plasma exchange or plasma infusion (PE/PI) therapy, which carries significant risks[29][30] and has not been proven effective in any controlled trials. People with aHUS and ESRD have also had to undergo lifelong dialysis, which has a 5-year survival rate of 34–38%.[31][32]
Pathogenesis
HUS is one of the thrombotic microangiopathies, a category of disorders that includes STEC-HUS, aHUS, and thrombotic thrombocytopenic purpura (TTP). STEC-HUS occurs after ingestion of a strain of bacteria expressing Shiga toxin(s), usually types of E. coli, that expresses verotoxin (also called Shiga-like toxin). E. coli can produce stx1 and/or stx2 Shiga toxins, the latter being more dangerous. A combination of both toxins in certain ratios is usually associated with HUS. These Shiga toxins bind GB3 receptors, globotriaosylceramide, which are present in renal tissue more than any other tissue and are also found in central nervous system neurons and other tissue. Children have more GB3 receptors than adults which may be why children are more susceptible to HUS. Cattle, swine, deer, and other mammals do not have GB3 receptors, but can be asymptomatic carriers of Shiga toxin-producing bacteria. Some humans can also be asymptomatic carriers. Once the bacteria colonizes, diarrhea followed by bloody diarrhea, hemorrhagic colitis, typically follows. STEC-HUS is usually preceded by a prodrome of diarrhea, which is often bloody, and is caused by Shiga-like toxin-producing bacteria such as enterohemorrhagic Escherichia coli (EHEC), of which E. coli O157:H7 is the most common serotype.[26] Other serotypes also cause disease and can emerge as new causes of STEC-HUS, as occurred with E. coli O104:H4, which triggered a 2011 epidemic of STEC-HUS in Germany.[33]
The typical pathophysiology of HUS involves the binding of Shiga-toxin to the globotriaosylceramide (Gb3; also called ceramide trihexoside which accumulates in Fabry disease) receptor on the surface of the glomerular endothelium.[34] This action includes a cascade of signaling events leading to apoptosis and binding of leukocytes to endothelial cells. The Shiga-toxin-activated endothelial cells then become thrombogenic (clot-producing) by a mechanism that is not fully understood,[35] though they have been shown to induce the release of cytokines and chemokines that are implicated in platelet activation.[36] Additionally, the binding action of Shiga-toxin inactivates a metalloproteinase called ADAMTS13, the deficiency of which causes the closely related TTP. Once ADAMTS13 is disabled, multimers of von Willebrand Factor (vWF) form and initiate platelet activation, causing microthrombus formation. The activation of platelets resulting from inhibition of ADAMTS13 is due to the hyperactivity of large multimers of uncleaved vWF. The arterioles and capillaries of the body become obstructed by the resulting complexes of activated platelets, which have adhered to the endothelium via large multimeric vWF. Through a mechanism known as microangiopathic hemolysis, the growing thrombi lodged in smaller vessels destroy red blood cells (RBCs) as they squeeze through the narrowed blood vessels, forming schistocytes, or fragments of sheared RBCs.[27] The presence of schistocytes is a key finding that helps to diagnose HUS. Typically, this hemolysis results in a hemoglobin level of less than 80g/L.
Shiga-toxin directly activates the alternative complement pathway and also interferes with complement regulation by binding to complement factor H, an inhibitor of the complement cascade. Shiga-toxin causes complement-mediated platelet, leukocyte, and endothelial cell activation, resulting in systemic hemolysis, inflammation and thrombosis.[37][38][39] Severe clinical complications of TMA have been reported in patients from 2 weeks to more than 44 days after presentation with STEC-HUS, with improvements in clinical condition extending beyond this time frame, suggesting that complement activation persists beyond the acute clinical presentation and for at least 4 months.[40]
The consumption of platelets as they adhere to the thrombi lodged in the small vessels typically leads to mild or moderate thrombocytopenia with a platelet count of less than 60,000 per microliter.[41] As in the related condition TTP, reduced blood flow through the narrowed blood vessels of the microvasculature leads to reduced blood flow to vital organs, and ischemia may develop.[10] The kidneys and the central nervous system (brain and spinal cord) are the parts of the body most critically dependent on high blood flow, and are thus the most likely organs to be affected. However, in comparison to TTP, the kidneys tend to be more severely affected in HUS, and the central nervous system is less commonly affected.[42]
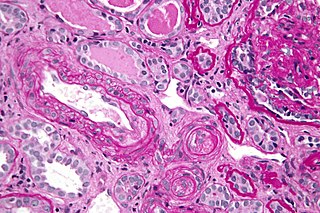
HUS occurs after 3–7% of all sporadic E. coli O157:H7 infections and up to approximately 20% or more of epidemic infections.[43] Children and adolescents are commonly affected.[44] Grossly, the kidneys may show patchy or diffuse renal cortical necrosis. Histologically, the glomeruli show thickened and sometimes split capillary walls due largely to endothelial swelling. Large deposits of fibrin-related materials in the capillary lumens, subendothelially, and in the mesangium are also found along with mesangiolysis. Interlobular and afferent arterioles show fibrinoid necrosis and intimal hyperplasia and are often occluded by thrombi.[11]
STEC-HUS most often affects infants and young children, but also occurs in adults. The most common form of transmission is ingestion of undercooked meat, unpasteurized fruits and juices, contaminated produce, contact with unchlorinated water, and person-to-person transmission in daycare or long-term care facilities.[24]
Unlike typical HUS, aHUS does not follow STEC infection and is thought to result from one or several genetic mutations that cause chronic, uncontrolled, and excessive activation of complement.[5] This leads to platelet activation, endothelial cell damage, and white blood cell activation, leading to systemic TMA, which manifests as decreased platelet count, hemolysis, damage to multiple organs, and ultimately, death.[6][17][27] Early signs of systemic complement-mediated TMA include thrombocytopenia (platelet count below 150,000 or a decrease from baseline of at least 25%)[15] and evidence of microangiopathic hemolysis, which is characterized by elevated LDH levels, decreased haptoglobin, decreased hemoglobin, and/or the presence of schistocytes.[6][28][15]
Diagnosis
The similarities between HUS, aHUS, and TTP make differential diagnosis essential.[6][28] All three of these systemic TMA-causing diseases are characterized by thrombocytopenia[15] and microangiopathic hemolysis,[5][15] plus one or more of the following: neurological symptoms (e.g., confusion,[5][23] cerebral convulsions,[23] seizures[20]); renal impairment[15] (e.g., elevated creatinine,[16] decreased estimated glomerular filtration rate [eGFR],[16] abnormal urinalysis[45]); and gastrointestinal (GI) symptoms (e.g., diarrhea,[18][21] nausea/vomiting,[20] abdominal pain,[20] gastroenteritis[15][18]).The presence of diarrhea does not exclude aHUS as the cause of TMA, as 28% of patients with aHUS present with diarrhea and/or gastroenteritis.[17][18] First diagnosis of aHUS is often made in the context of an initial, complement-triggering infection, and Shiga-toxin has also been implicated as a trigger that identifies patients with aHUS.[40] Additionally, in one study, mutations of genes encoding several complement regulatory proteins were detected in 8 of 36 (22%) patients diagnosed with STEC-HUS.[46] However, the absence of an identified complement regulatory gene mutation does not preclude aHUS as the cause of the TMA, as approximately 50% of patients with aHUS lack an identifiable mutation in complement regulatory genes.[18]
Diagnostic work-up supports the differential diagnosis of TMA-causing diseases. A positive Shiga-toxin/EHEC test confirms a cause for STEC-HUS,[24][26] and severe ADAMTS13 deficiency (i.e., ≤5% of normal ADAMTS13 levels) confirms a diagnosis of TTP.[47]
Prevention
The effect of antibiotics in shiga toxin producing E. coli is unclear.[1] While some early studies raised concerns more recent studies show either no effect or a benefit.[1]
While eculizumab is being used to treat atypical hemolytic uremic syndrome, no evidence as of 2018 supports its use in the main forms of HUS.[1] Scientists are trying to understand how useful it would be to immunize humans or cattle.[48]
Prognosis
Acute renal failure occurs in 55–70% of people with STEC-HUS, although up to 70–85% recover renal function.[49] Patients with aHUS generally have poor outcomes, with up to 50% progressing to ESRD or irreversible brain damage; as many as 25% die during the acute phase.[49] However, with aggressive treatment, more than 90% of patients survive the acute phase of HUS, and only about 9% may develop ESRD. Roughly one-third of persons with HUS have abnormal kidney function many years later, and a few require long-term dialysis. Another 8% of persons with HUS have other lifelong complications, such as high blood pressure, seizures, blindness, paralysis, and the effects of having part of their colon removed. The overall mortality rate from HUS is 5–15%. Children and the elderly have a worse prognosis.[50]
Epidemiology
The country with the highest incidence of HUS is Argentina[51][52][53][54] and it performs a key role in the research of this condition.
In the United States, the overall incidence of HUS is estimated at 2.1 cases per 100,000 persons/year, with a peak incidence between six months and four years of age.[55]
HUS and the E. coli infections that cause it have been the source of much negative publicity for the FDA, meat industries, and fast-food restaurants since the 1990s, especially in the contaminations linked to Jack in the Box restaurants. In 2006, an epidemic of harmful E. coli emerged in the United States due to contaminated spinach. In June, 2009, NestléToll House cookie dough was linked to an outbreak of E. coli O157:H7 in the United States, which sickened 70 people in 30 states.[55]
In May, 2011 an epidemic of bloody diarrhea caused by E. coli O104:H4-contaminated fenugreek seeds hit Germany. Tracing the epidemic revealed more than 3,800 cases, with HUS developing in more than 800 of the cases, including 36 fatal cases. Nearly 90% of the HUS cases were in adults.[56][57]
Related Research Articles
Thrombotic thrombocytopenic purpura (TTP) is a blood disorder that results in blood clots forming in small blood vessels throughout the body. This results in a low platelet count, low red blood cells due to their breakdown, and often kidneys, heart, and brain dysfunction. Symptoms may include large bruises, fever, weakness, shortness of breath, confusion, and headache. Repeated episodes may occur.
Uremia is the condition of having high levels of urea in the blood. Urea is one of the primary components of urine. It can be defined as an excess of amino acid and protein metabolism end products, such as urea and creatinine, in the blood that would be normally excreted in the urine. Uremic syndrome can be defined as the terminal clinical manifestation of kidney failure. It is the signs, symptoms and results from laboratory tests which result from inadequate excretory, regulatory and endocrine function of the kidneys. Both uremia and uremic syndrome have been used interchangeably to denote a very high plasma urea concentration that is the result of renal failure. The former denotation will be used for the rest of the article.
Microangiopathic hemolytic anemia (MAHA) is a microangiopathic subgroup of hemolytic anemia caused by factors in the small blood vessels. It is identified by the finding of anemia and schistocytes on microscopy of the blood film.
von Willebrand factor (VWF) is a blood glycoprotein involved in hemostasis. It is deficient and or defective in von Willebrand disease and is involved in many other diseases, including thrombotic thrombocytopenic purpura, Heyde's syndrome, and possibly hemolytic-uremic syndrome. Increased plasma levels in many cardiovascular, neoplastic, and connective tissue diseases are presumed to arise from adverse changes to the endothelium, and may predict an increased risk of thrombosis.
Hemoglobinuria is a condition in which the oxygen transport protein hemoglobin is found in abnormally high concentrations in the urine. The condition is often associated with any hemolytic anemia with primarily intravascular hemolysis, in which red blood cells (RBCs) are destroyed, thereby releasing free hemoglobin into the plasma. Excess hemoglobin is filtered by the kidneys, which excrete it into the urine, giving urine a purple color. Hemoglobinuria can lead to acute tubular necrosis which is an uncommon cause of a death of uni-traumatic patients recovering in the ICU.
A schistocyte or schizocyte is a fragmented part of a red blood cell. Schistocytes are typically irregularly shaped, jagged, and have two pointed ends.
The AB5 toxins are six-component protein complexes secreted by certain pathogenic bacteria known to cause human diseases such as cholera, dysentery, and hemolytic-uremic syndrome. One component is known as the A subunit, and the remaining five components are B subunits. All of these toxins share a similar structure and mechanism for entering targeted host cells. The B subunit is responsible for binding to receptors to open up a pathway for the A subunit to enter the cell. The A subunit is then able to use its catalytic machinery to take over the host cell's regular functions.
Escherichia coli O121 is a pathogenic serotype of Escherichia coli, associated with Shiga toxin, intestinal bleeding, and hemolytic-uremic syndrome (HUS). HUS, if left untreated, can lead to kidney failure.
Complement factor I, also known as C3b/C4b inactivator, is a protein that in humans is encoded by the CFI gene. Complement factor I is a protein of the complement system, first isolated in 1966 in guinea pig serum, that regulates complement activation by cleaving cell-bound or fluid phase C3b and C4b. It is a soluble glycoprotein that circulates in human blood at an average concentration of 35 μg/mL.
Enteroinvasive Escherichia coli (EIEC) is a type of pathogenic bacteria whose infection causes a syndrome that is identical to shigellosis, with profuse diarrhea and high fever. EIEC are highly invasive, and they use adhesin proteins to bind to and enter intestinal cells. They produce no toxins, but severely damage the intestinal wall through mechanical cell destruction.
A novel strain of Escherichia coli O104:H4 bacteria caused a serious outbreak of foodborne illness focused in northern Germany in May through June 2011. The illness was characterized by bloody diarrhea, with a high frequency of serious complications, including hemolytic-uremic syndrome (HUS), a condition that requires urgent treatment. The outbreak was originally thought to have been caused by an enterohemorrhagic (EHEC) strain of E. coli, but it was later shown to have been caused by an enteroaggregative E. coli (EAEC) strain that had acquired the genes to produce Shiga toxins, present in organic fenugreek sprouts.
Escherichia coli O104:H4 is an enteroaggregative Escherichia coli strain of the bacterium Escherichia coli, and the cause of the 2011 Escherichia coli O104:H4 outbreak. The "O" in the serological classification identifies the cell wall lipopolysaccharide antigen, and the "H" identifies the flagella antigen.
Shigatoxigenic Escherichia coli (STEC) and verotoxigenic E. coli (VTEC) are strains of the bacterium Escherichia coli that produce either Shiga toxin or Shiga-like toxin (verotoxin). Only a minority of the strains cause illness in humans. The ones that do are collectively known as enterohemorrhagic E. coli (EHEC) and are major causes of foodborne illness. When infecting humans, they often cause gastroenteritis, enterocolitis, and bloody diarrhea and sometimes cause a severe complication called hemolytic-uremic syndrome (HUS). The group and its subgroups are known by various names. They are distinguished from other strains of intestinal pathogenic E. coli including enterotoxigenic E. coli (ETEC), enteropathogenic E. coli (EPEC), enteroinvasive E. coli (EIEC), enteroaggregative E. coli (EAEC), and diffusely adherent E. coli (DAEC).
Antimotility agents are drugs used to alleviate the symptoms of diarrhea. These include loperamide (Imodium), diphenoxylate with atropine (Lomotil), and opiates such as paregoric, tincture of opium, codeine, and morphine. In diarrhea caused by invasive pathogens such as Salmonella, Shigella, and Campylobacter, the use of such agents has generally been strongly discouraged, though evidence is lacking that they are harmful when administered in combination with antibiotics in Clostridium difficile cases. Use of antimotility agents in children and the elderly has also been discouraged in treatment of EHEC due to an increased rate of hemolytic uremic syndrome.
Escherichia coli is a gram-negative, rod-shaped bacterium that is commonly found in the lower intestine of warm-blooded organisms (endotherms). Most E. coli strains are harmless, but pathogenic varieties cause serious food poisoning, septic shock, meningitis, or urinary tract infections in humans Unlike normal flora E. coli, the pathogenic varieties produce toxins and other virulence factors that enable them to reside in parts of the body normally not inhabited by E. coli and to damage host cells. These pathogenic traits are encoded by virulence genes carried only by the pathogens.
Atypical hemolytic uremic syndrome (aHUS) is an extremely rare, life-threatening, progressive disease that frequently has a genetic component. In most cases it can be effectively controlled with Soliris (eculizimab). Current treatment with Soliris breaks the complement cascade and often allows significant recovery from aHUS' otherwise detrimental effects.
↑ Gasser C, Gautier E, Steck A, Siebenmann RE, Oechslin R (September 1955). "Hemolytic-uremic syndrome: bilateral necrosis of the renal cortex in acute acquired hemolytic anemia". Schweiz Med Wochenschr (in German). 85 (38–39): 905–9. PMID13274004.
1 2 Ståhl, A.-L.; Vazir-Sani, F.; Heinen, S.; et al. (2008). "Factor H dysfunction in patients with atypical hemolytic uremic syndrome contributes to complement deposition on platelets and their activation". Blood. 111 (11): 5307–5317. doi:10.1182/blood-2007-08-106153. PMID18268093.
1 2 3 4 Zipfel, PF; Heinen, S; Skerka, C (2010). "Thrombotic microangiopathies: new insights and new challenges". Current Opinion in Nephrology and Hypertension. 19 (4): 372–378. doi:10.1097/MNH.0b013e32833aff4a. PMID20539230.
↑ European Renal Association- European Dialysis and Transplant Association Registry (2011). ERA-EDTA Registry Annual Report 2009. Amsterdam, The Netherlands: Academic Medical Center Department of Medical Informatics.
1 2 Mache, C; et al. (June 2010). "Eculizumab in diarrhea-associated hemolytic uremic syndrome". Presented at the 2nd International Conference on HUS-MPGN-PNH.
↑ Chu, P; Hemphill, RR (2004). "222: Acquired hemolytic anemia". Emergency Medicine: A Comprehensive Study Guide (6th ed.). New York, NY: McGraw-Hill. ISBN978-0-07-138875-7.
↑ Rivero, MA; Passucci, JA; Rodriguez, EM; Signorini, ML; Tarabla, HD; Parma, AE (2011). "Factors associated with sporadic verotoxigenic Escherichia coli infection in children with diarrhea from the Central Eastern Area of Argentina". Foodborne Pathogens and Disease. 8 (8): 901–6. doi:10.1089/fpd.2010.0800. PMID21492023.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.