No treatments can stop or reverse its progression, though some may temporarily improve symptoms.[2] A healthy diet, physical activity, and social engagement are generally beneficial in aging, and may help in reducing the risk of cognitive decline and Alzheimer's.[20] Affected people become increasingly reliant on others for assistance, often placing a burden on caregivers.[24] The pressures can include social, psychological, physical, and economic elements.[24] Exercise programs may be beneficial with respect to activities of daily living and can potentially improve outcomes.[25] Behavioral problems or psychosis due to dementia are sometimes treated with antipsychotics, but this has an increased risk of early death.[26][27]
As of 2020, there were approximately 50 million people worldwide with Alzheimer's disease.[14] It most often begins in people over 65years of age, although up to 10% of cases are early-onset impacting those in their 30s to mid-60s.[28][4] It affects about 6% of people 65 years and older,[17] and women more often than men.[29] The disease is named after German psychiatrist and pathologist Alois Alzheimer, who first described it in 1906.[30] Alzheimer's financial burden on society is large, with an estimated global annual cost of US$1trillion.[14] Alzheimer's and related dementias are ranked as the seventh leading cause of death worldwide.[31]
Given the widespread impacts of Alzheimer's disease, both basic-science and health funders in many countries support Alzheimer's research at large scales. For example, the US National Institutes of Health program for Alzheimer's research, the National Plan to Address Alzheimer's Disease, has a budget of US$3.98 billion for fiscal year 2026.[32] In the European Union, the 2020 Horizon Europe research programme awarded over €570 million for dementia-related projects.[33]
Signs and symptoms
The course of Alzheimer's is generally described in three stages, with a progressive pattern of cognitive and functionalimpairment.[34][28] The three stages are described as early or mild, middle or moderate, and late or severe.[34] The disease is known to target the hippocampus which is associated with memory, and this is responsible for the first symptoms of memory impairment. As the disease progresses so does the degree of memory impairment.[20]
The first symptoms are often mistakenly attributed to aging or stress.[35] Detailed neuropsychological testing can reveal mild cognitive difficulties up to eight years before a person fulfills the clinical criteria for diagnosis of Alzheimer's disease.[36] These early symptoms can affect the most complex activities of daily living.[37] The most noticeable deficit is short term memory loss, which shows up as difficulty in remembering recently learned facts and inability to acquire new information.[36]
Subtle problems with the executive functions of attentiveness, planning, flexibility, and abstract thinking, or impairments in semantic memory (memory of meanings, and concept relationships) can also be symptomatic of the early stages of Alzheimer's disease.[36]Apathy and depression can be seen at this stage, with apathy remaining as the most persistent symptom throughout the course of the disease.[38][39] People with objective signs of cognitive impairment, but not more severe symptoms, may be diagnosed with mild cognitive impairment (MCI). If memory loss is the predominant symptom of MCI, it is termed amnestic MCI and is frequently seen as a prodromal or early stage of Alzheimer's disease.[40] Amnestic MCI has a greater than 90% likelihood of being associated with Alzheimer's.[41]
Early stage
In people with Alzheimer's disease, the increasing impairment of learning and memory eventually leads to a definitive diagnosis. In a small percentage, difficulties with language, executive functions, perception (agnosia), or execution of movements (apraxia) are more prominent than memory problems.[42] Alzheimer's disease does not affect all memory capacities equally. Older memories of the person's life (episodic memory), facts learned (semantic memory), and implicit memory (the memory of the body on how to do things, such as using a fork to eat or how to drink from a glass) are affected to a lesser degree than new facts or memories.[43][44]
Language problems are mainly characterised by a shrinking vocabulary and decreased word fluency, leading to a general impoverishment of oral and written language.[42][45] In this stage, the person with Alzheimer's is usually capable of communicating basic ideas adequately.[42][45][46] While performing fine motor tasks such as writing, drawing, or dressing, certain movement coordination and planning difficulties (apraxia) may be present; however, they are commonly unnoticed.[42] As the disease progresses, people with Alzheimer's disease can often continue to perform many tasks independently; however, they may need assistance or supervision with the most cognitively demanding activities.[42]
Middle stage
Progressive deterioration eventually hinders independence, with subjects being unable to perform most common activities of daily living.[42] Speech difficulties become evident due to an inability to recall vocabulary, which leads to frequent incorrect word substitutions (paraphasias). Reading and writing skills are also progressively lost.[42][46] Complex motor sequences become less coordinated as time passes and Alzheimer's disease progresses, so the risk of falling increases.[42] During this phase, memory problems worsen, and the person may fail to recognise close relatives.[42]Long-term memory, which was previously intact, becomes impaired.[42]
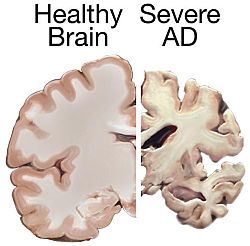
A normal brain on the left and a late-stage Alzheimer's brain on the right
During the final stage, known as the late-stage or severe stage, there is complete dependence on caregivers.[20][34][42] Language is reduced to simple phrases or even single words, eventually leading to complete loss of speech.[42][46] Despite the loss of verbal language abilities, people can often understand and return emotional signals. Although aggressiveness can still be present, extreme apathy and exhaustion are much more common symptoms. People with Alzheimer's disease will ultimately not be able to perform even the simplest tasks independently; muscle mass and mobility deteriorates to the point where they are bedridden and unable to feed themselves.[49] The cause of death is usually an external factor, such as infection of pressure ulcers or pneumonia, not the disease itself.[42] In some cases, there is a paradoxical lucidity immediately before death, where there is an unexpected recovery of mental clarity.[50]
Causes
Alzheimer's disease is believed to occur when abnormal amounts of amyloid beta (Aβ), accumulating extracellularly as amyloid plaques and tau proteins, or intracellularly as neurofibrillary tangles, form in the brain, affecting neuronal functioning and connectivity, resulting in a progressive loss of brain function.[51][52] This altered protein clearance ability is age-related, regulated by brain cholesterol,[53] and associated with other neurodegenerative diseases.[54][55]
The cause for most Alzheimer's cases is still mostly unknown,[14] except for 1–2% of cases where deterministic genetic differences have been identified.[18] Several competing hypotheses attempt to explain the underlying cause; the most predominant hypothesis is the amyloid beta (Aβ) hypothesis.[14]
Genetic
Late onset
Late-onset Alzheimer's is about 70% heritable.[56][57] Most cases of Alzheimer's are not familial, and so they are termed sporadic Alzheimer's disease.[58] Of the cases of sporadic Alzheimer's disease, most are classified as late onset where they are developed after the age of 65 years.[59]
The strongest genetic risk factor for sporadic Alzheimer's disease is APOEε4.[19] APOEε4 is one of four alleles of apolipoprotein E (APOE). APOE plays a major role in lipid-binding proteins in lipoprotein particles and the ε4 allele disrupts this function.[60] Between 40% and 80% of people with Alzheimer's disease possess at least one APOEε4 allele.[61] The APOEε4 allele increases the risk of the disease by three times in heterozygotes and by 15 times in homozygotes.[62] Like many human diseases, environmental effects and genetic modifiers result in incomplete penetrance. For example, Nigerian Yoruba people do not show the relationship between dose of APOEε4 and incidence or age-of-onset for Alzheimer's disease seen in other human populations.[63][64]
Only 1–2% of Alzheimer's cases are inherited due to autosomal dominant effects, as Alzheimer's is highly polygenic. When the disease is caused by autosomal dominant variants, it is known as early onset familial Alzheimer's disease, which is rarer and has a faster rate of progression.[18] Less than 5% of sporadic Alzheimer's disease have an earlier onset,[18] and early-onset Alzheimer's is about 90% heritable.[56][57] Familial Alzheimer's disease usually implies two or more persons affected in one or more generations.[65][66][67]
Early onset familial Alzheimer's disease can be attributed to mutations in one of three genes: those encoding amyloid-beta precursor protein (APP) and presenilinsPSEN1 and PSEN2.[41] Most mutations in the APP and presenilin genes increase the production of a small protein called amyloid beta (Aβ)42, which is the main component of amyloid plaques.[68] Some of the mutations merely alter the ratio between Aβ42 and the other major forms—particularly Aβ40—without increasing Aβ42 levels in the brain.[69] Two other genes associated with autosomal dominant Alzheimer's disease are ABCA7 and SORL1.[70]
Alleles in the TREM2 gene have been associated with a three to five times higher risk of developing Alzheimer's disease.[71]
A Japanese pedigree of familial Alzheimer's disease was found to be associated with a deletion mutation of codon 693 of APP.[72] This mutation and its association with Alzheimer's disease was first reported in 2008,[73] and is known as the Osaka mutation. Only homozygotes with this mutation have an increased risk of developing Alzheimer's disease. This mutation accelerates Aβ oligomerization but the proteins do not form the amyloid fibrils that aggregate into amyloid plaques, suggesting that it is the Aβ oligomerization rather than the fibrils that may be the cause of this disease. Mice expressing this mutation have all the usual pathologies of Alzheimer's disease.[74]
Hypotheses
Misfolded protein
Tau protein abnormalities in neurons may contribute to onset of Alzheimer's disease
Two abnormal proteins define the pathology of Alzheimer's disease: amyloid beta protein (Aβ) in amyloid plaques and tau protein in neurofibrillary tangles.[1] These proteins share two features that promote their ability to cause disease: They both become abnormal by misfolding, that is, by assuming a shape that is rich in beta sheets;[75] and they proliferate in the brain by the prion-like mechanism of seeded protein aggregation.[76][77] The presence of these abnormal proteins in Alzheimer's disease has spawned two hypotheses of the proteopathic origin of the disease: The amyloid (or Aβ) hypothesis, and the tau hypothesis.
The amyloid hypothesis, also known as the "amyloid cascade hypothesis"[78][79] or "Aβ cascade hypothesis",[80] holds that the accumulation of misfolded Aβ in the brain is the fundamental cause of Alzheimer's disease. In the amyloid cascade, the buildup of abnormal Aβ leads to tauopathy and eventually the complex degenerative changes of advanced Alzheimer's disease.[81] Abnormal Aβ is thought to damage the brain by directly interacting with cells, and/or indirectly, for example by causing oxidative stress and neuroinflammation.[82]
The amyloid hypothesis is supported by evidence from genetics and biomarkers. All autosomal dominant genetic causes of Alzheimer's disease affect either the amyloid precursor protein (APP) on chromosome 21 or the enzymes that generate Aβ, known as presenilin 1 and presenilin 2. In addition, people with trisomy 21 (Down syndrome), most of whom have an extra copy of the gene for APP, almost universally develop the symptoms and neuropathology of Alzheimer's disease by 40 years of age.[10][83] Conversely, people with a rare mutation in the APP gene that reduces the production of Aβ and its tendency to aggregate are protected against Alzheimer's disease.[83] Additionally, a major genetic risk factor for Alzheimer's disease is a specific isoform of apolipoprotein E, APOE4.[16] Of the three major isoforms (APOE2, APOE3 and APOE4), APOE4 is linked to the least efficient removal of Aβ by astrocytes, which promotes the buildup of Aβ in the brain. The most efficient clearance of Aβ is achieved by cells bearing the APOE2 isoform, which protects against Alzheimer's disease.[83] Evidence from biomarkers such as imaging of protein deposits in the brain and measurement of brain-derived substances in cerebrospinal fluid and blood implicates abnormalities of Aβ as the earliest and most robust disease-specific change in Alzheimer's disease.[84]
The tau hypothesis proposes that abnormalities of the tau protein initiate the disease cascade, at least in cases of idiopathic Alzheimer's disease.[85] The tau hypothesis is supported by the histopathological findings of Heiko Braak and colleagues that tauopathy can be detected in certain neurons before Aβ plaques are evident.[85] Specifically, Alzheimer's starts with the hyperphosphorylation of tau in specific vulnerable neuronal populations such as the locus coeruleus and projection neurons of the association cortex. There is agreement in the research community that tau contributes strongly to dementia in Alzheimer's disease, but tauopathy occurs in over 30 diseases besides Alzheimer's disease).[86] In addition, mutations of the gene for tau (MAPT) cause neurodegenerative disorders known as primary tauopathies, but these diseases occur in the absence of Aβ proteopathy.[83] Current evidence thus favors abnormal Aβ as the prime mover of Alzheimer's disease.[83][87] However, the Aβ hypothesis and tau hypothesis are not mutually exclusive, in that abnormalities of Aβ initiate the disease and tauopathy is required for its complete expression.[88][89]
Hormonal
Because women have a higher incidence of AD than men, it has been thought that estrogen deficiency during menopause is a risk factor. In a 2025 analysis of the Canadian Longitudinal Study on Aging earlier age at menopause was linked with lower cognitive performance.[90]
Infection
The possibility that infectious agents cause Alzheimer's disease has been considered since the early 20th century, when Oskar Fischer likened amyloid plaques to small masses (called 'Drusen') of a microbe called actinomyces.[91] Since then, at least 15 different agents, including bacteria, viruses, fungi and protozoa, have been proposed to cause Alzheimer's disease.[92] No definitive evidence has been presented that a specific infectious agent is necessary and sufficient to cause Alzheimer's disease.[93] However, it is possible that microbial infections might act as risk factors for the disease.[94] For example, human herpes viruses such as HSV1, HHV6 and HHV7 have been linked to the risk of Alzheimer's disease.[93] In addition, some pathogens have been reported to seed Aβ deposition in the brain,[93] and aggregated Aβ has antimicrobial properties, suggesting that Aβ plaques might form when brain cells generate Aβ to fight infection.[94] Researchers caution that brain infections can cause dementia by mechanisms unrelated to Alzheimer's disease.[94][93]
The cholinergic hypothesis proposes that the loss of neurons in the basal forebrain, which produce the neurotransmitter acetylcholine, is a key event in the pathogenesis of Alzheimer's disease.[96] These cells supply acetylcholine to synapses in the limbic system and cerebral cortex.[40][96] The cholinergic hypothesis led to the development of drugs that increase acetylcholine in the brains of Alzheimer patients.[96] The efficacy of these agents is limited, probably because many other neurotransmitter systems degenerate in Alzheimer's disease.[97]
Sleep
Sleep disturbances are seen as a possible risk factor for inflammation in Alzheimer's disease.[98] Sleep disruption was previously only seen as a consequence of Alzheimer's disease, but as of 2020[update], accumulating evidence suggests that this relationship may be bidirectional.[99][100]
Neuroinflammation, metal toxicity, smoking, and air pollution
Systemic markers of the innate immune system are risk factors for late-onset Alzheimer's disease,[101] and misfolded Aβ and tau proteins both are associated with oxidative stress and neuroinflammation.[102] Chronic inflammation also is a feature of other neurodegenerative diseases, including Parkinson's disease, and ALS.[103] The cellular homeostasis of biometals such as ionic copper, iron, and zinc is disrupted in Alzheimer's disease, though it remains unclear whether this is produced by or causes the changes in proteins.[14][104] Smoking is a significant Alzheimer's disease risk factor.[1]Exposure to air pollution may be a contributing factor to the development of Alzheimer's disease.[14]
Age-related myelin decline
Retrogenesis is a medical hypothesis that just as the fetus goes through a process of neurodevelopment beginning with neurulation and ending with myelination, the brains of people with Alzheimer's disease go through a reverse neurodegeneration process starting with demyelination and death of axons (white matter) and ending with the death of grey matter.[105] Likewise the hypothesis is, that as infants go through states of cognitive development, people with Alzheimer's disease go through the reverse process of progressive cognitive impairment.[106]
The association with celiac disease is unclear, with a 2019 study finding no increase in dementia overall in those with celiac disease while a 2018 review found an association with several types of dementia including Alzheimer's disease.[110][111]
Studies have reported a potential link between infection with certain viruses and developing Alzheimer's disease later in life.[112] Notably, a large scale study conducted on 6,245,282 patients has reported an increased risk of developing Alzheimer's disease following COVID-19 infection in cognitively normal individuals over 65.[113]
Some evidence suggests that some viral infections such as Herpes simplex virus 1 (HSV-1) may be associated with dementia, but there are conflicting results and the association with Alzheimer's is unclear as of 2024.[114][115][116]
Some researchers have proposed that Alzheimer's disease is Type 3 diabetes because of a number of correspondences with both Type 1 and Type 2 diabetes.[117]
The gross (macroscopic) appearance of the brain in Alzheimer's disease is variable. In many cases the cortical sulci are widened and the gyri are shrunken,[118] but the degree of cortical atrophy varies, and it can sometimes be difficult to discern, particularly in very old subjects.[119] The areas most affected by atrophy are the medial temporal lobe including the hippocampal formation, the amygdala, the frontal lobe and the parietal lobe; the occipital lobe is relatively unaffected by atrophy.[118] The volume of the ventricles increases in parallel with cortical shrinkage.[118] Studies using MRI and PET have documented reductions in the size of specific brain regions in people with Alzheimer's disease as they progress from mild cognitive impairment to Alzheimer's disease, and in comparison with similar images from healthy older adults.[120][121] These macroscopic changes in the brain can occur in other disorders and to some extent in normal aging; thus, they are not specific to Alzheimer's disease, which can be diagnosed with certainty only by microscopic examination of the brain.[119]
At the microscopic level, the defining histopathologic characteristics of Alzheimer's disease are abundant Aβplaques and neurofibrillary tangles in certain brain regions.[122] Both of these abnormalities are clearly visible by microscopy;[123][118] in the early stages of disease, tangles are present mainly in the medial temporal lobe and plaques are present mainly in the neocortex, but as the disease progresses the lesions proliferate throughout much of the brain.[122] Although it was once thought that Alzheimer's disease can occur without neurofibrillary tangles in the neocortex,[124] newer methods have shown that dementia in these cases can be linked to a comorbid condition, often Lewy body disease.[86]
Aβ plaques are dense, mostly insoluble deposits of amyloid beta peptide and cellular material outside and around neurons.[94] Neurofibrillary tangles are aggregates of the microtubule-associated protein tau which has become hyperphosphorylated and accumulates inside neurons.[125][122] Although many older individuals develop some plaques and tangles as a consequence of aging, the brains of people with Alzheimer's disease have a greater number of them in specific brain regions.[126][118]
The two defining proteopathies of Alzheimer's disease: Aβ plaques (brown) and neurofibrillary (tau) tangles (black). Abnormal, hyperphosphorylated tau occurs in neuronal cell bodies, in fine neuronal processes throughout the neuropil, and in swollen neurites within the plaques. Dual immunohistochemical stain using antibodies to Aβ and tau proteins. Scale bar = 50 microns (0.05 mm).
In addition to plaques and tangles, other neuropathological changes contribute to the clinicopathologic features of advanced Alzheimer's disease. These include cerebral Aβ-amyloid angiopathy (CAA),[127] inflammation,[128] and the loss of neurons[129] and synapses.[130] The disappearance of neurons and their synapses is a particularly prominent correlate of dementia, although not all cells are affected equally. Selective vulnerability - that is, why certain neurons and synapses are affected and others spared - is an important unanswered question.[130][129]
In more than half of the cases examined neuropathologically, and especially in very old people, the pathology of Alzheimer's disease is accompanied by lesions that are characteristic of other brain disorders.[122] The most common of these comorbid conditions are vascular disease, Lewy body disease, and TDP-43 proteinopathy.[122][131] This mixed pathology can complicate both diagnosis and the evaluation of clinical trials,[122] which often target only one of several potential contributors to dementia.
Alzheimer's disease has been identified as a protein misfolding disease, a proteopathy, caused by the accumulation of abnormally folded Aβ protein into amyloid plaques, and tau protein into neurofibrillary tangles in the brain.[132] Plaques are made up of small peptides, 39–43amino acids in length, called Aβ. Aβ is a fragment derived from the larger Aβ precursor protein (APP), a transmembrane protein that penetrates the cell's membrane. APP is critical to neuronal growth, survival, and post-injury repair.[132] In Alzheimer's disease, the enzymes gamma secretase and beta secretase act together in a proteolytic process that divides APP into smaller fragments.[132] One of these fragments is Aβ, which misfolds and self-assembles into fibrils; these fibrils form clumps that deposit outside neurons in dense formations known as Aβ plaques.[132] Excitatory neurons are known to be major producers of Aβ that contribute to extracellular plaque deposition.[132]
Enzymes act on the amyloid-beta precursor protein and cut it into fragments. The beta-amyloid fragment is crucial in the formation of amyloid plaques in Alzheimer's disease.
Phosphorylated tau
Alzheimer's disease is also considered a tauopathy due to the abnormal aggregation of the tau protein within cells. Every neuron has a cytoskeleton, an internal support structure partly made up of organelles called microtubules. These microtubules act like tracks, guiding nutrients and molecules from the body of the cell to the ends of the axon and back. The tau protein stabilises the microtubules when phosphorylated, and it is therefore called a microtubule-associated protein. In Alzheimer's disease, tau undergoes chemical changes, becoming hyperphosphorylated; it then begins to pair with other threads, creating neurofibrillary tangles and disintegrating the neuron's transport system.[133] Pathogenic tau can also cause neuronal death through transposable element dysregulation.[134]Necroptosis has also been reported as a mechanism of cell death in brain cells affected with tau tangles.[135][136]
Disease mechanism
Exactly how disturbances of production and aggregation of the Aβ peptide give rise to the pathology of Alzheimer's disease is not known.[137][138] The amyloid hypothesis (also known as the 'amyloid cascade hypothesis') posits that the accumulation of abnormally shaped Aβ peptides is the central event triggering the sequence of changes that eventually lead to neurodegeneration and dementia.[139] Misfolded Aβ accumulates in the brain because it causes normal Aβ molecules to similarly misfold by a prion-like 'seeding' mechanism.[140][141][142] The aggregated Aβ takes the form of small oligomers (which are particularly toxic to neurons[143][144][139]) and amyloid fibrils, the long polymers that are the main components of Aβ plaques.[94] Some researchers have argued that the amyloid fibrils bind up smaller oligomers and thus protect brain cells from the injurious effects of the oligomers.[144] However, the plaques are not benign inasmuch as they are associated with abnormal neuronal processes and local inflammation.[122] Whatever the relative influence of Aβ oligomers and fibrils, the presence of aggregated Aβ is associated with the disruption of neuronal metabolism[145] and various other changes such as inflammation.[122][94] Aβ also selectively builds up in mitochondria in the cells of Alzheimer's-affected brains, and it inhibits certain enzyme functions and the utilisation of glucose by neurons.[146]
Evidence supports Aβ as playing a central role in the pathogenesis of Alzheimer's disease, but as the disease progresses the brain undergoes a complex assortment of cellular and molecular changes, including (in addition to tauopathy) inflammation, oxidative/nitrative stress, DNA damage, epigenetic changes, excitotoxicity, endosomal/lysosomal failure, dysproteostasis, autophagy failure, lipid dysmetabolism, calcium ion (Ca2+) dyshomeostasis, post-translational protein modifications, neuronal cell cycle re-entry, mitochondrial failure, cytoskeletal disruption, glucose dysmetabolism, vascular or lymphatic impairments, and biometal dyshomeostasis.[147] Iron dyshomeostasis is linked to disease progression in which an iron-dependent form of regulated cell death called ferroptosis could be involved. Products of lipid peroxidation are also elevated in the Alzheimer brain compared with controls.[148]
Various inflammatory processes and cytokines also play a role in the pathology of Alzheimer's disease. Inflammation is a general marker of tissue damage in any disease, and may be either secondary to tissue damage in Alzheimer's disease or a marker of an immunological response.[149] Cells that mediate neuroinflammation in Alzheimer's include microglia, astrocytes, oligodendrocytes, lymphocytes and myeloid cells.[128] There is increasing evidence of a strong interaction between neurons and the immunological mechanisms in the brain. Obesity and systemic inflammation may interfere with immunological processes which promote disease progression.[150]Microglia are especially important actors in the Alzheimer's-related inflammation.[151] Microglia are the principal immunological cells of the central nervous system, serving as the tissue-resident macrophages of the brain; they are capable of recognizing and taking up Aβ through multiple pattern recognition receptors, making them central to amyloid clearance within the brain.[152] However, microglia can also be a major source of pro-inflammatory mediators which can be deleterious to neurological function.[152] Microglia are topographically associated with aberrant deposits of tau and Aβ within the brain, even when each pathologic component occurs in distinct brain regions.[153] Microglial activation has been documented in people with mild cognitive impairment, despite a lack of detectable binding of a PET tracer for Aβ in the brain, suggesting that microglial dysfunction may precede plaque deposition as an inciting event in AD.[154]
By the time the symptoms of Alzheimer's first appear, the complex degenerative mechanisms in the brain have been active for many years. Hence, the beneficial effect of therapeutics (specifically, the monoclonal antibodies that promote Aβ clearance) has ranged from nonexistent to modest.[157] Second-generation antibodies to Aβ have resulted in significant slowing of the progression of Alzheimer's disease,[158] but these have not yet stopped or reversed dementia. Hence, researchers increasingly believe that the best strategy is to prevent Alzheimer's by intervening before the brain has been irreversibly damaged.[159][160]
PET scan of the brain of a person with Alzheimer's disease showing a loss of function in the temporal lobe
Alzheimer's disease (AD) can only be definitively diagnosed with autopsy findings; in the absence of autopsy, clinical diagnoses of AD are "possible" or "probable", based on other findings.[22][23][161] Up to 23% of those clinically diagnosed with AD may be misdiagnosed and may have pathology suggestive of another condition with symptoms that mimic those of AD.[23]
AD is usually clinically diagnosed based on a person's medical history, observations from friends or relatives, and behavioral changes. The presence of characteristic neuropsychological changes with impairments in at least two cognitive domains that are severe enough to affect a person's functional abilities are required for the diagnosis. Domains that may be impaired include memory (most commonly impaired), language, executive function, visuospatial functioning, or other areas of cognition. The neurocognitive changes must be a decline from a prior level of function and the diagnosis requires ruling out other common causes of neurocognitive decline.[162][163][164] Advanced medical imaging with computed tomography (CT) or magnetic resonance imaging (MRI), and with single-photon emission computed tomography (SPECT) or positron emission tomography (PET), can be used to help exclude other cerebral pathology or subtypes of dementia.[165] On MRI or CT, Alzheimer's disease usually shows a generalised or focal cortical atrophy, which may be asymmetric. Atrophy of the hippocampus is also commonly seen. Brain imaging commonly also shows cerebrovascular disease, most commonly previous strokes (small or large territory strokes), and this is thought to be a contributing cause of many cases of dementia (up to 46% cases of dementia also have cerebrovascular disease on imaging).[162] FDG-PET scan is not required for the diagnosis but it is sometimes used when standard testing is unclear. FDG-PET shows a bilateral, asymmetric, temporal and parietal reduced activity.[162] Advanced imaging may predict conversion from prodromal stages (mild cognitive impairment) to Alzheimer's disease.[166] FDA-approved radiopharmaceutical diagnostic agents used in PET for Alzheimer's disease are florbetapir (2012), flutemetamol (2013), florbetaben (2014), and flortaucipir (2020).[167] Because many insurance companies in the United States do not cover this procedure, its use in clinical practice is largely limited to clinical trials as of 2018[update].[168]
Assessment of intellectual functioning including memory testing can further characterise the state of the disease.[1] Medical organizations have created diagnostic criteria to ease and standardise the diagnostic process for practising physicians. Definitive diagnosis can only be confirmed with post-mortem evaluations when brain material is available and can be examined histologically for senile plaques and neurofibrillary tangles.[168][169]
The DSM-5 defines criteria for probable or possible AD for both major and mild neurocognitive disorder.[171][172][161] Major or mild neurocognitive disorder must be present along with at least one cognitive deficit for a diagnosis of either probable or possible AD.[171][173] For major neurocognitive disorder due to AD, probable Alzheimer's disease can be diagnosed if the individual has genetic evidence of AD[174] or if two or more acquired cognitive deficits, and a functional disability that is not from another disorder, are present.[175] Otherwise, possible AD can be diagnosed as the diagnosis follows an atypical route.[173] For mild neurocognitive disorder due to AD, probable Alzheimer's disease can be diagnosed if there is genetic evidence, whereas possible AD can be met if all of the following are present: no genetic evidence, decline in both learning and memory, two or more cognitive deficits, and a functional disability not from another disorder.[171][176]
The NIA-AA criteria are used mainly in research rather than in clinical assessments.[177] They define AD through three major stages: preclinical, mild cognitive impairment (MCI), and Alzheimer's dementia.[178][179] Diagnosis in the preclinical stage is complex and focuses on asymptomatic individuals;[179][180] the latter two stages describe individuals experiencing symptoms,[179] along with biomarkers,[181] predominantly those for neuronal injury (mainly tau-related) and amyloid beta deposition.[177][179] The core clinical criteria itself rests on the presence of cognitive impairment[179] without the presence of comorbidities.[182][183] The third stage is divided into probable and possible AD dementia.[183] In probable AD dementia there is steady impairment of cognition over time and a memory-related or non-memory-related cognitive dysfunction.[183] In possible AD dementia, another causal disease such as cerebrovascular disease is present.[183]
Techniques
Cognitive tests such as the mini–mental state examination (MMSE) can help in the diagnosis of Alzheimer's disease. In this test instructions are given to copy drawings like the one reported, remember some words, read, and subtract numbers serially.
Neuropsychological tests including cognitive tests such as the mini–mental state examination (MMSE), the Montreal Cognitive Assessment (MoCA) and the Mini-Cog are widely used to aid in diagnosis of the cognitive impairments in AD.[184] These tests may not always be accurate, as they lack sensitivity to mild cognitive impairment, and can be biased by language or attention problems;[184] more comprehensive test arrays are necessary for high reliability of results, particularly in the earliest stages of the disease.[185][186]
Further neurological examinations are crucial in the differential diagnosis of Alzheimer's disease and other diseases.[35] Interviews with family members are used in assessment, and caregivers can supply important information on daily living abilities and on the decrease in the person's mental function.[187] A caregiver's viewpoint is particularly important, since a person with Alzheimer's disease is commonly unaware of their deficits.[188] Many times, families have difficulties in the detection of initial dementia symptoms and may not communicate accurate information to a physician.[189]
Supplemental testing can rule out other potentially treatable diagnoses and help avoid misdiagnoses.[190] Common supplemental tests include blood tests, thyroid function tests, as well as tests to assess vitamin B12 levels, rule out neurosyphilis and rule out metabolic problems (including tests for kidney function, electrolyte levels and for diabetes).[190] MRI or CT scans might also be used to rule out other potential causes of the symptoms – including tumors or strokes.[184]Delirium and depression can be common among individuals and are important to rule out.[191]
Due to low accuracy, the C-PIB-PET scan is not recommended as an early diagnostic tool or for predicting the development of AD when people show signs of mild cognitive impairment (MCI).[195] The use of 18F-FDG PET scans, as a single test, to identify people who may develop Alzheimer's disease is not supported by evidence.[196]
In May 2025, the US FDA approved a blood test by Fujirebio Diagnostics' Lumipulse G pTau217/ß-Amyloid 1-42 Plasma Ratio diagnostic device for the early detection of amyloid plaques associated with AD in adults aged 55 years and older who are exhibiting signs and symptoms of the disease.[197]
Prevention
Intellectual activities such as playing chess or regular social interaction have been linked to a reduced risk of Alzheimer's disease in epidemiological studies, although no causal relationship has been found.
There is no disease-modifying treatments proven to cure Alzheimer's disease and because of this, AD research has focused on interventions to prevent the onset and progression.[13] There is no evidence that supports any particular measure in preventing AD,[1] and studies of measures to prevent the onset or progression have produced inconsistent results. Epidemiological studies have proposed relationships between an individual's likelihood of developing AD and modifiable factors, such as medications, lifestyle, and diet. There are some challenges in determining whether interventions for AD act as a primary prevention method, preventing the disease itself, or a secondary prevention method, identifying the early stages of the disease.[198] These challenges include duration of intervention, different stages of disease at which intervention begins, and lack of standardization of inclusion criteria regarding biomarkers specific for AD.[198] Further research is needed to determine factors that can help prevent AD.[198]
Medication
Cardiovascular risk factors, such as hypercholesterolaemia, hypertension, diabetes, and smoking, are associated with a higher risk of onset and worsened course of AD.[199][200] The use of statins to lower cholesterol may be of benefit in AD.[201]Antihypertensive and antidiabetic medications in individuals without overt cognitive impairment may decrease the risk of dementia by influencing cerebrovascular pathology.[1][202] More research is needed to examine the relationship with AD specifically; clarification of the direct role medications play versus other concurrent lifestyle changes (diet, exercise, smoking) is needed.[1]
Depression is associated with an increased risk for AD; management with antidepressant medications may provide a preventative measure.[5]
Historically, long-term usage of non-steroidal anti-inflammatory drugs (NSAIDs) were thought to be associated with a reduced likelihood of developing AD as it reduces inflammation, but NSAIDs do not appear to be useful as a treatment.[168] Additionally, because women have a higher incidence of AD than men, it was once thought that estrogen deficiency during menopause was a risk factor, but there is a lack of evidence to show that hormone replacement therapy (HRT) in menopause decreases risk of cognitive decline.[203]
Certain lifestyle activities, such as physical and cognitive exercises, higher education and occupational attainment, cigarette smoking, stress, sleep, and the management of other comorbidities, including diabetes and hypertension, may affect the risk of developing AD.[5]
Physical exercise is associated with a decreased rate of dementia,[6] and is effective in reducing symptom severity in those with AD.[204][205] Memory and cognitive functions can be improved with aerobic exercises including brisk walking three times weekly for forty minutes.[206] It may also induce neuroplasticity of the brain.[207] Participating in mental exercises, such as reading, crossword puzzles, and chess have reported potential to be preventive.[5] Meeting the WHO recommendations for physical activity is associated with a lower risk of AD.[208]
Higher education and occupational attainment, and participation in leisure activities, contribute to a reduced risk of developing AD,[7] or of delaying the onset of symptoms. This is compatible with the cognitive reserve theory, which states that some life experiences result in more efficient neural functioning providing the individual a cognitive reserve that delays the onset of dementia manifestations.[7]Education delays the onset of Alzheimer's disease syndrome without changing the duration of the disease.[209]
Cessation in smoking may reduce risk of developing AD, specifically in those who carry the APOE ɛ4 allele.[209][5] The increased oxidative stress caused by smoking results in downstream inflammatory or neurodegenerative processes that may increase risk of developing AD.[210] Avoidance of smoking, counseling and pharmacotherapies to quit smoking are used, and avoidance of environmental tobacco smoke is recommended.[5]
Alzheimer's disease is associated with sleep disorders but the precise relationship is unclear.[211][212] It was once thought that as people get older, the risk of developing sleep disorders and AD independently increase, but research suggests sleep disorders may be a risk factor for AD.[213] One theory is that the mechanisms to increase clearance of toxic substances, including Aβ, are active during sleep.[211][214] With decreased sleep, a person is increasing Aβ production and decreasing Aβ clearance, resulting in Aβ accumulation.[98][211][212] Receiving adequate sleep (approximately 7–8 hours) every night has become a potential lifestyle intervention to prevent the development of AD.[5]
Stress is a risk factor for the development of AD.[5] The mechanism by which stress predisposes someone to development of AD is unclear, but it is suggested that lifetime stressors may affect a person's epigenome, leading to an overexpression or under expression of specific genes.[215] Although the relationship of stress and AD is unclear, strategies to reduce stress and relax the mind may be helpful strategies in preventing the progression or Alzheimer's disease.[216] Meditation, for instance, is a helpful lifestyle change to support cognition and well-being, though further research is needed to assess long-term effects.[207]
Reduction in the activity of the cholinergic neurons is a well-known feature of AD.[222] Acetylcholinesterase inhibitors are employed to reduce the rate at which the body breaks down acetylcholine (ACh), thereby increasing the concentration of ACh in the brain and combating the loss of ACh caused by the death of cholinergic neurons.[223] Evidence supports medical efficacy in mild to moderate AD,[224][219] and somewhat in the advanced stage.[219] This does not extend to delaying symptom onset.[225]
An extract of Ginkgo biloba known as EGb 761 has been used for treating AD and other neuropsychiatric disorders.[231] Its use is approved throughout Europe.[232] A 2016 review concluded that the quality of evidence from clinical trials on G. biloba has been insufficient to warrant its use.[233]
Atypical antipsychotics are modestly useful in reducing aggression and psychosis in people with AD, but their advantages are offset by serious adverse effects, such as stroke, movement difficulties or cognitive decline.[234] They are recommended in dementia only after first line therapies such as behavior modification have failed, and due to the risk of adverse effects, they should be used for the shortest amount of time possible.[162] Stopping antipsychotic use in this group of people appears to be safe.[235]
Side effects
The most common side effects are nausea and vomiting, both of which are linked to cholinergic excess. These side effects arise in approximately 10–20% of users, are mild to moderate in severity, and can be managed by slowly adjusting medication doses.[236] Less common secondary effects include muscle cramps, decreased heart rate (bradycardia), decreased appetite and weight, and increased gastric acid production.[224] Reported adverse events with memantine are infrequent and mild, including hallucinations, confusion, dizziness, headache and fatigue.[237]
Antibodies
Two antibodies have been approved to target amyloid beta – donanemab and lecanemab[238][239][240] – but as of 2025, their role in treatment is uncertain because of side effects, questions about efficacy, and cost.[241]
Psychosocial interventions are used as an adjunct to pharmaceutical treatment and can be classified within behavior-, emotion-, cognition- or stimulation-oriented approaches.[needs update][246]
Behavioral interventions attempt to identify and reduce the antecedents and consequences of problem behaviors. This approach has not reported success in improving overall functioning,[247] but can help to reduce some specific problem behaviors, such as incontinence.[248] There is a lack of high quality data on the effectiveness of these techniques in other behavior problems such as wandering.[249][250]Music therapy is effective in reducing behavioral and psychological symptoms.[251]
Emotion-oriented interventions include reminiscence therapy, validation therapy, supportive psychotherapy, sensory integration, also called snoezelen, and simulated presence therapy. A Cochrane review has found no evidence that this is effective.[252] Reminiscence therapy (RT) involves the discussion of past experiences individually or in group, many times with the aid of photographs, household items, music and sound recordings, or other familiar items from the past. A 2018 review of the effectiveness of RT found that effects were inconsistent, small in size and of doubtful clinical significance, and varied by setting.[253] Simulated presence therapy (SPT) is based on attachment theories and involves playing a recording with voices of the closest relatives of the person with AD. There is partial evidence indicating that SPT may reduce challenging behaviors.[254]
The aim of cognition-oriented treatments, which include reality orientation and cognitive retraining, is the reduction of cognitive deficits. Reality orientation consists of the presentation of information about time, place, or person to ease the understanding of the person about its surroundings and his or her place in them. On the other hand, cognitive retraining tries to improve impaired capacities by exercising mental abilities. Both have reported some efficacy improving cognitive capacities.[255]
Stimulation-oriented treatments include art, music and pet therapies, exercise, and any other kind of recreational activities. Stimulation has modest support for improving behavior, mood, and, to a lesser extent, function. Nevertheless, as important as these effects are, the main support for the use of stimulation therapies is the change in the person's routine.[246]
Since AD has no cure and it gradually renders people incapable of tending to their own needs, caregiving is essentially the treatment and must be carefully managed over the course of the disease.
During the early and moderate stages, modifications to the living environment and lifestyle can increase safety and reduce caretaker burden.[256][257] Examples of such modifications are the adherence to simplified routines, the placing of safety locks, the labeling of household items to cue the person with the disease or the use of modified daily life objects.[246][258][259] If eating becomes problematic, food will need to be prepared in smaller pieces or even puréed.[260] When swallowing difficulties arise, the use of feeding tubes may be required. In such cases, the medical efficacy and ethics of continuing feeding is an important consideration of the caregivers and family members.[261][262] The use of physical restraints is rarely indicated in any stage of the disease, although there are situations when they are necessary to prevent harm to the person with Alzheimer's disease or their caregivers.[246]
During the final stages of the disease, treatment is centred on relieving discomfort until death, often with the help of hospice.[263]
Diet
Diet may be a modifiable risk factor for the development of Alzheimer's disease but more research needs to be conducted.[264] The Mediterranean diet, and the DASH diet are both associated with less cognitive decline.[265] A different approach has been to incorporate elements of both of these diets into one known as the MIND diet.[265] Results from large-scale epidemiological studies and clinical trials have not demonstrated an independent role for most individual dietary components.[265]
Prognosis
The early stages of AD are difficult to diagnose.[266] A definitive diagnosis is usually made once cognitive impairment compromises daily living activities, although the person may still be living independently. The symptoms will progress from mild cognitive problems, such as memory loss through increasing stages of cognitive and non-cognitive disturbances, eliminating any possibility of independent living, especially in the late stages of the disease.[42]
Life expectancy of people with AD is reduced.[267] The normal life expectancy for 60 to 70 years old is 23 to 15 years; for 90 years old it is 4.5 years.[268] Following AD diagnosis it ranges from 7 to 10 years for those in their 60s and early 70s (a loss of 13 to 8 years), to only about 3 years or less (a loss of 1.5 years) for those in their 90s.[267]
As of 1995, fewer than 3% of people live more than fourteen years after diagnosis.[269] Disease features significantly associated with reduced survival are increased severity of cognitive impairment, decreased functional level, disturbances in the neurological examination, history of falls, malnutrition, dehydration and weight loss.[3] Other coincident diseases such as heart problems, diabetes, or history of alcohol abuse are also related with shortened survival.[270][271][272] While the earlier the age at onset the higher the total survival years, life expectancy is particularly reduced when compared to the healthy population among those who are younger.[273]
Men have a less favorable survival prognosis than women, even after controlling for age and some medical conditions.[274][275] As of 2025, the reasons for the higher mortality in men are unknown. It has been speculated that men have different dementia risk factors than women, like traumatic brain injury.[275]
Aspiration pneumonia is the most frequent immediate cause of death brought by AD.[3] While the reasons behind the lower prevalence of cancer in AD patients remain unclear, some researchers hypothesize that biological mechanisms shared by both diseases might play a role. However, this requires further investigation.[276]
Regarding incidence, where a disease-free population is followed over the years have shown rates between 10 and 15 per thousand person-years for all dementias and 5–8 for AD in Spain and Italy,[277][278] which means that half of new dementia cases each year are Alzheimer's disease. Advancing age is a primary risk factor for the disease and incidence rates are not equal for all ages: every 5 years after the age of 65, the risk of acquiring the disease approximately doubles, increasing from 3 to as much as 69 per thousand person years.[277][278] The prevalence of AD in populations is dependent upon factors including incidence and survival. Since the incidence of AD increases with age, prevalence depends on the mean age of the population for which prevalence is given. In the United States in 2020, AD dementia prevalence was estimated to be 5.3% for those in the 60–74 age group, with the rate increasing to 13.8% in the 74–84 group and to 34.6% in those greater than 85.[279] Prevalence rates in some less developed regions around the globe are lower.[280][281] Both the prevalence and incidence rates of AD are steadily increasing, and the prevalence rate is estimated to triple by 2050 reaching 152 million, compared to the 50 million people with AD globally in 2020.[bettersourceneeded][14][282][bettersourceneeded][283]
Sex difference
Women with AD are more common than males.[29] This difference has been thought to be due to women's longer life spans. According to one study when adjusted for age, both sexes were affected by Alzheimer's at equal rates.[16] However, many studies have found even higher age-adjusted numbers for women, including the Framingham study which found women to have almost twice the lifetime risk of men.[29]
As of 2025 it is unknown why women are more commonly affected by AD, although many theories exist as mentioned in the section causes above. There are also observable differences in the disease course, as tau protein accumulates faster in women than in men.[284] Also, presence of APOE4 increases AD risk more in women than in men.[285] Even if the same amount of AD pathology observed in a woman compared to a man, there is greater cognitive decline in a woman.[286]
This is relevant for therapy, like the timing of anti-tau treatments[284] or menopausal hormone therapy: In the Canadian Longitudinal Study of Aging women on MHT had higher memory scores than those who were not on MHT.[90]
Ethnicity
In the United States, the risk of dying from AD in 2010 was 26% higher among the non-Hispanic white population than among the non-Hispanic black population, and the Hispanic population had a 30% lower risk than the non-Hispanic white population.[287] However, much AD research remains to be done in minority groups, such as the African American, East Asian and Hispanic/Latino populations.[288][289] Studies have reported that these groups are underrepresented in clinical trials and do not have the same risk of developing AD when carrying certain genetic risk factors (i.e. APOE4), compared to their caucasian counterparts.[289][290][291]
History
Alois Alzheimer's patient Auguste Deter in 1902. Hers was the first described case of what became known as Alzheimer's disease.
The ancient Greek and Roman philosophers and physicians associated old age with increasing dementia.[30] It was not until 1901 that German psychiatrist Alois Alzheimer identified the first case of what became known as Alzheimer's disease, named after him, in a fifty-year-old woman he called Auguste D. He followed her case until she died in 1906 when he first reported publicly on it.[292] During the next five years, eleven similar cases were reported in the medical literature, some of them already using the term Alzheimer's disease.[30] The disease was first described as a distinctive disease by Emil Kraepelin after suppressing some of the clinical (delusions and hallucinations) and pathological features (arteriosclerotic changes) contained in the original report of Auguste D.[293] He included Alzheimer's disease, also named preseniledementia by Kraepelin, as a subtype of senile dementia in the eighth edition of his Textbook of Psychiatry, published on 15 July 1910.[294]
For most of the 20th century, the diagnosis of Alzheimer's disease was reserved for individuals between the ages of 45 and 65 who developed symptoms of dementia. The terminology changed after 1977 when a conference on Alzheimer's disease concluded that the clinical and pathological manifestations of presenile and senile dementia were almost identical, although the authors also added that this did not rule out the possibility that they had different causes.[295] This eventually led to the diagnosis of Alzheimer's disease independent of age.[296] The term senile dementia of the Alzheimer type (SDAT) was used for a time to describe the condition in those over 65, with classical Alzheimer's disease being used to describe those who were younger. Eventually, the term Alzheimer's disease was formally adopted in medical nomenclature to describe individuals of all ages with a characteristic common symptom pattern, disease course, and neuropathology.[297]
Dementia, and specifically Alzheimer's disease, may be among the most costly diseases for societies worldwide.[301] As populations age, these costs will probably increase and become an important social problem and economic burden.[302] Costs associated with AD include direct and indirect medical costs, which vary between countries depending on social care for a person with AD.[301][303][304] Direct costs include doctor visits, hospital care, medical treatments, nursing home care, specialised equipment, and household expenses.[301][302] Indirect costs include the cost of informal care and the loss in productivity of informal caregivers.[302]
In the United States as of 2019[update], informal (family) care is estimated to constitute nearly three-fourths of caregiving for people with AD at a cost of US$234 billion per year and approximately 18.5 billion hours of care.[301] The cost to society worldwide to care for individuals with AD is projected to increase nearly ten-fold, and reach about US$9.1 trillion by 2050.[303]
Costs for those with more severe dementia or behavioral disturbances are higher and are related to the additional caregiving time to provide physical care.[304]
This section needs to be updated. Please help update this article to reflect recent events or newly available information.(February 2022)
Individuals with Alzheimer's will require assistance in their lifetime, and care will most likely come in the form of a full-time caregiver which is often a role that is taken on by the spouse or a close relative. Caregiving tends to include physical and emotional burdens as well as time and financial strain at times on the person administering the aid.[305][306] Alzheimer's disease is known for placing a great burden on caregivers which includes social, psychological, physical, or economic aspects.[24][307][308] Home care is usually preferred by both those people with Alzheimer's disease as well as their families.[309] This option also delays or eliminates the need for more professional and costly levels of care.[309][310] Nevertheless, two-thirds of nursing home residents have dementias.[246]
Dementia caregivers are subject to high rates of physical and mental disorders.[311] Factors associated with greater psychosocial problems of the primary caregivers include having an affected person at home, the caregiver being a spouse, demanding behaviors of the cared person such as depression, behavioral disturbances, hallucinations, sleep problems or walking disruptions and social isolation.[312][313] In the United States, the yearly cost of caring for a person with dementia ranges from $28,078-$56,022 per year for formal medical care and $36,667-$92,689 for informal care provided by a relative or friend (assuming market value replacement costs for the care provided by the informal caregiver) and $15,792-$71,813 in lost wages.[314]
Specific medications that may reduce the risk or progression of Alzheimer's disease include those that impact Aβplaques, inflammation, APOE, neurotransmitter receptors, neurogenesis, growth factors or hormones.[329][330][331]
123Todd S, Barr S, Roberts M, Passmore AP (November 2013). "Survival in dementia and predictors of mortality: a review". International Journal of Geriatric Psychiatry. 28 (11): 1109–1124. doi:10.1002/gps.3946. PMID23526458.
123Berchtold NC, Cotman CW (1998). "Evolution in the conceptualization of dementia and Alzheimer's disease: Greco-Roman period to the 1960s". Neurobiology of Aging. 19 (3): 173–189. doi:10.1016/S0197-4580(98)00052-9. PMID9661992. S2CID24808582.
↑Nygård L (2003). "Instrumental activities of daily living: a stepping-stone towards Alzheimer's disease diagnosis in subjects with mild cognitive impairment?". Acta Neurologica Scandinavica. Supplementum. 179 (s179): 42–46. doi:10.1034/j.1600-0404.107.s179.8.x. PMID12603250. S2CID25313065.
12Taler V, Phillips NA (July 2008). "Language performance in Alzheimer's disease and mild cognitive impairment: a comparative review". Journal of Clinical and Experimental Neuropsychology. 30 (5): 501–556. doi:10.1080/13803390701550128. PMID18569251. S2CID37153159.
123Frank EM (September 1994). "Effect of Alzheimer's disease on communication function". Journal of the South Carolina Medical Association. 90 (9): 417–423. PMID7967534.
↑Volicer L, Harper DG, Manning BC, Goldstein R, Satlin A (May 2001). "Sundowning and circadian rhythms in Alzheimer's disease". The American Journal of Psychiatry. 158 (5): 704–711. doi:10.1176/appi.ajp.158.5.704. PMID11329390. S2CID10492607.
↑Gold DP, Reis MF, Markiewicz D, Andres D (January 1995). "When home caregiving ends: a longitudinal study of outcomes for caregivers of relatives with dementia". Journal of the American Geriatrics Society. 43 (1): 10–16. doi:10.1111/j.1532-5415.1995.tb06235.x. PMID7806732. S2CID29847950.
↑Mashour GA, Frank L, Batthyany A, Kolanowski AM, Nahm M, Schulman-Green D, etal. (August 2019). "Paradoxical lucidity: A potential paradigm shift for the neurobiology and treatment of severe dementias". Alzheimer's & Dementia. 15 (8): 1107–1114. doi:10.1016/j.jalz.2019.04.002. hdl:2027.42/153062. PMID31229433. S2CID195063786.
↑Tomiyama T (July 2010). "[Involvement of beta-amyloid in the etiology of Alzheimer's disease]". Brain and Nerve = Shinkei Kenkyu No Shinpo. 62 (7): 691–699. PMID20675873.
↑Tomiyama T, Nagata T, Shimada H, Teraoka R, Fukushima A, Kanemitsu H, etal. (March 2008). "A new amyloid beta variant favoring oligomerization in Alzheimer's-type dementia". Annals of Neurology. 63 (3): 377–387. doi:10.1002/ana.21321. PMID18300294. S2CID42311988.
↑Goedert M (2015). "NEURODEGENERATION. Alzheimer's and Parkinson's diseases: The prion concept in relation to assembled Aβ, tau, and α-synuclein". Science. 349 (6248) 1255555. doi:10.1126/science.1255555. PMID26250687.
↑Hardy J, Allsop D (October 1991). "Amyloid deposition as the central event in the aetiology of Alzheimer's disease". Trends in Pharmacological Sciences. 12 (10): 383–388. doi:10.1016/0165-6147(91)90609-V. PMID1763432.
1234Itzhaki R, Golde TE, Heneka MT, Readhead B (April 2020). "Do infections have a role in the pathogenesis of Alzheimer disease?". Nature Reviews Neurology. 16 (4): 193–197. doi:10.1038/s41582-020-0323-9. PMID32152461.
↑Eikelenboom P, van Exel E, Hoozemans JJ, Veerhuis R, Rozemuller AJ, van Gool WA (2010). "Neuroinflammation – an early event in both the history and pathogenesis of Alzheimer's disease". Neuro-Degenerative Diseases. 7 (1–3): 38–41. doi:10.1159/000283480. PMID20160456. S2CID40048333.
↑Reisberg B, Franssen EH, Hasan SM, Monteiro I, Boksay I, Souren LE, etal. (1999). "Retrogenesis: clinical, physiologic, and pathologic mechanisms in brain aging, Alzheimer's and other dementing processes". European Archives of Psychiatry and Clinical Neuroscience. 249 (3): 28–36. doi:10.1007/pl00014170. PMID10654097. S2CID23410069.
↑Luczynski P, Laule C, Hsiung GR, Moore GR, Tremlett H (January 2019). "Coexistence of Multiple Sclerosis and Alzheimer's disease: A review". Multiple Sclerosis and Related Disorders. 27: 232–238. doi:10.1016/j.msard.2018.10.109. PMID30415025.
↑Makhlouf S, Messelmani M, Zaouali J, Mrissa R (March 2018). "Cognitive impairment in celiac disease and non-celiac gluten sensitivity: review of literature on the main cognitive impairments, the imaging and the effect of gluten free diet". Acta Neurologica Belgica (Review). 118 (1): 21–27. doi:10.1007/s13760-017-0870-z. PMID29247390. S2CID3943047.
↑Biagio P, Isabella DF, Federica C, Elena S, Ivan G (May 2024). "Alzheimer's disease and herpes viruses: Current events and perspectives". Rev Med Virol. 34 (3) e2550. doi:10.1002/rmv.2550. PMID38801246.
12345Duyckaerts C, Lowe J, Frosch M (2014). "Pathology of degenerative diseases of the nervous system". In Gray F, Duyckaerts C, De Girolami U (eds.). Basic Neuropathology. Oxford University Press. pp.173–204. ISBN978-0-19-992905-4.
↑Tiraboschi P, Sabbagh MN, Hansen LA, Salmon DP, Merdes A, Gamst A, etal. (April 2004). "Alzheimer disease without neocortical neurofibrillary tangles: "a second look"". Neurology. 62 (7): 1141–1147. doi:10.1212/01.wnl.0000118212.41542.e7. PMID15079014. S2CID22832110.
↑Hauw JJ, Duyckaerts C (2001). "Alzheimer's disease". In Duckett S, DeLaTorre JC (eds.). Pathology of the Aging Human Nervous System. Oxford University Press. pp.207–263. ISBN0-19-513069-3.
↑Bouras C, Hof PR, Giannakopoulos P, Michel JP, Morrison JH (1994). "Regional distribution of neurofibrillary tangles and senile plaques in the cerebral cortex of elderly patients: a quantitative evaluation of a one-year autopsy population from a geriatric hospital". Cerebral Cortex. 4 (2): 138–150. doi:10.1093/cercor/4.2.138. PMID8038565.
↑Kotzbauer PT, Trojanowsk JQ, Lee VM (October 2001). "Lewy body pathology in Alzheimer's disease". Journal of Molecular Neuroscience. 17 (2): 225–232. doi:10.1385/JMN:17:2:225. PMID11816795. S2CID44407971.
↑Van Broeck B, Van Broeckhoven C, Kumar-Singh S (2007). "Current insights into molecular mechanisms of Alzheimer disease and their implications for therapeutic approaches". Neuro-Degenerative Diseases. 4 (5): 349–365. doi:10.1159/000105156. PMID17622778. S2CID7949658.
↑Leng F, Edison P (March 2021). "Neuroinflammation and microglial activation in Alzheimer disease: where do we go from here?". Nat Rev Neurol. 17 (3): 157–172. doi:10.1038/s41582-020-00435-y. PMID33318676.
↑Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th Text Revisioned.). Washington, DC: American Psychiatric Association. 2000. ISBN978-0-89042-025-6.
123Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C.: American Psychiatric Association. 2013. p.611. ISBN978-0-89042-555-8.
↑Sachs-Ericsson N, Blazer DG (January 2015). "The new DSM-5 diagnosis of mild neurocognitive disorder and its relation to research in mild cognitive impairment". Aging & Mental Health. 19 (1): 2–12. doi:10.1080/13607863.2014.920303. PMID24914889. S2CID46244321.
↑Harvey PD, Moriarty PJ, Kleinman L, Coyne K, Sadowsky CH, Chen M, etal. (2005). "The validation of a caregiver assessment of dementia: the Dementia Severity Scale". Alzheimer Disease and Associated Disorders. 19 (4): 186–194. doi:10.1097/01.wad.0000189034.43203.60. PMID16327345. S2CID20238911.
↑Antoine C, Antoine P, Guermonprez P, Frigard B (2004). "[Awareness of deficits and anosognosia in Alzheimer's disease]". L'Encéphale (in French). 30 (6): 570–577. doi:10.1016/S0013-7006(04)95472-3. PMID15738860.
↑Cruz VT, Pais J, Teixeira A, Nunes B (2004). "[The initial symptoms of Alzheimer disease: caregiver perception]". Acta Médica Portuguesa (in Portuguese). 17 (6): 435–444. PMID16197855.
123Stern SD, Cifu AS, Altkorn D (2020). Symptom to diagnosis: an evidence-based guide (4thed.). New York: McGraw-Hill Medical. pp.209–210. ISBN978-1-260-12111-7. OCLC1121597721.
↑Jha A, Mukhopadhaya K (2021). Alzheimer's disease: diagnosis and treatment guide. Cham, Switzerland: Springer. p.32. ISBN978-3-030-56739-2. OCLC1202472277.
↑Rosendorff C, Beeri MS, Silverman JM (2007). "Cardiovascular risk factors for Alzheimer's disease". The American Journal of Geriatric Cardiology. 16 (3): 143–149. doi:10.1111/j.1076-7460.2007.06696.x. PMID17483665.
↑Lacerda RA, Desio JA, Kammers CM, Henkes S, Freitas de Sá M, de Souza EF, etal. (November 2024). "Sleep disorders and risk of alzheimer's disease: A two-way road". Ageing Res Rev. 101 102514. doi:10.1016/j.arr.2024.102514. PMID39317268.
↑Fink HA, Linskens EJ, MacDonald R, Silverman PC, McCarten JR, Talley KM, etal. (May 2020). "Benefits and Harms of Prescription Drugs and Supplements for Treatment of Clinical Alzheimer-Type Dementia". Annals of Internal Medicine. 172 (10): 656–668. doi:10.7326/M19-3887. PMID32340037. S2CID216595473.
↑Berkowitz A (2017). Clinical neurology and neuroanatomy: a localization-based approach. New York: McGraw Hill. p.236. ISBN978-1-259-83440-0. OCLC948547621.
↑Geula C, Mesulam MM (1995). "Cholinesterases and the pathology of Alzheimer disease". Alzheimer Disease and Associated Disorders. 9 (Suppl 2): 23–28. doi:10.1097/00002093-199501002-00005. PMID8534419.
↑Raina P, Santaguida P, Ismaila A, Patterson C, Cowan D, Levine M, etal. (March 2008). "Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline". Annals of Internal Medicine. 148 (5): 379–397. doi:10.7326/0003-4819-148-5-200803040-00009. PMID18316756. S2CID22235353.
↑Yang G, Wang Y, Sun J, Zhang K, Liu J (22 October 2015). "Ginkgo Biloba for Mild Cognitive Impairment and Alzheimer's Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials". Current Topics in Medicinal Chemistry. 16 (5): 520–528. doi:10.2174/1568026615666150813143520. PMID26268332.
↑Declercq T, Petrovic M, Azermai M, Vander Stichele R, De Sutter AI, van Driel ML, etal. (March 2013). "Withdrawal versus continuation of chronic antipsychotic drugs for behavioural and psychological symptoms in older people with dementia". The Cochrane Database of Systematic Reviews. 3 (3) CD007726. doi:10.1002/14651858.CD007726.pub2. hdl:1854/LU-3109108. PMID23543555.
↑Alldredge BK, Corelli RL, Ernst ME, Guglielmo BJ, Jacobson PA, Kradjan WA, etal. (2013). Applied therapeutics: the clinical use of drugs (10thed.). Baltimore: Wolters Kluwer Health/Lippincott Williams & Wilkins. p.2385. ISBN978-1-60913-713-7.
12345[needs update]Rabins PV, Blacker D, Rovner BW, Rummans T, Schneider LS, Tariot PN, etal. (Steering Committee on Practice Guidelines) (December 2007). "American Psychiatric Association practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Second edition". The American Journal of Psychiatry. 164 (12 Suppl): 5–56. PMID18340692.
↑Bottino CM, Carvalho IA, Alvarez AM, Avila R, Zukauskas PR, Bustamante SE, etal. (December 2005). "Cognitive rehabilitation combined with drug treatment in Alzheimer's disease patients: a pilot study". Clinical Rehabilitation. 19 (8): 861–869. doi:10.1191/0269215505cr911oa. PMID16323385. S2CID21290731.
12Zanetti O, Solerte SB, Cantoni F (2009). "Life expectancy in Alzheimer's disease (AD)". Archives of Gerontology and Geriatrics. 49 (Suppl 1): 237–243. doi:10.1016/j.archger.2009.09.035. PMID19836639.
↑Mölsä PK, Marttila RJ, Rinne UK (March 1995). "Long-term survival and predictors of mortality in Alzheimer's disease and multi-infarct dementia". Acta Neurologica Scandinavica. 91 (3): 159–164. doi:10.1111/j.1600-0404.1995.tb00426.x. PMID7793228. S2CID19724937.
↑Bowen JD, Malter AD, Sheppard L, Kukull WA, McCormick WC, Teri L, etal. (August 1996). "Predictors of mortality in patients diagnosed with probable Alzheimer's disease". Neurology. 47 (2): 433–439. doi:10.1212/wnl.47.2.433. PMID8757016. S2CID24961809.
↑Jagger C, Clarke M, Stone A (January 1995). "Predictors of survival with Alzheimer's disease: a community-based study". Psychological Medicine. 25 (1): 171–177. doi:10.1017/S0033291700028191. PMID7792352. S2CID34066330.
↑Lanni C, Masi M, Racchi M, Govoni S (January 2021). "Cancer and Alzheimer's disease inverse relationship: an age-associated diverging derailment of shared pathways". Molecular Psychiatry. 26 (1): 280–295. doi:10.1038/s41380-020-0760-2. PMID32382138.
12Bermejo-Pareja F, Benito-León J, Vega S, Medrano MJ, Román GC (January 2008). "Incidence and subtypes of dementia in three elderly populations of central Spain". Journal of the Neurological Sciences. 264 (1–2): 63–72. doi:10.1016/j.jns.2007.07.021. PMID17727890. S2CID34341344.
12Di Carlo A, Baldereschi M, Amaducci L, Lepore V, Bracco L, Maggi S, etal. (January 2002). "Incidence of dementia, Alzheimer's disease, and vascular dementia in Italy. The ILSA Study". Journal of the American Geriatrics Society. 50 (1): 41–48. doi:10.1046/j.1532-5415.2002.50006.x. PMID12028245. S2CID22576935.
↑Li F, Qin W, Zhu M, Jia J (1 January 2021). "Model-Based Projection of Dementia Prevalence in China and Worldwide: 2020-2050". Journal of Alzheimer's Disease. 82 (4). IOS Press: 1823–1831. doi:10.3233/JAD-210493. PMID34219732. S2CID235735045.
↑Massett HA, Mitchell AK, Alley L, Simoneau E, Burke P, Han SH, etal. (29 June 2021). "Facilitators, Challenges, and Messaging Strategies for Hispanic/Latino Populations Participating in Alzheimer's Disease and Related Dementias Clinical Research: A Literature Review". Journal of Alzheimer's Disease. 82 (1): 107–127. doi:10.3233/JAD-201463. PMID33998537. S2CID234745473.
Alzheimer A (1907). "Über eine eigenartige Erkrankung der Hirnrinde" [About a peculiar disease of the cerebral cortex]. Allgemeine Zeitschrift für Psychiatrie und Psychisch-Gerichtlich Medizin (in German). 64 (1–2): 146–148.
Alzheimer A (1987). "About a peculiar disease of the cerebral cortex. By Alois Alzheimer, 1907". Alzheimer Disease and Associated Disorders. 1 (1). Translated by L. Jarvik, H. Greenson: 3–8. PMID3331112.
↑Kraepelin E (2007). Clinical Psychiatry: A Textbook For Students And Physicians (Reprint). Translated by Diefendorf AR. Kessinger Publishing. p.568. ISBN978-1-4325-0833-3.
↑Katzman R, Terry RD, Bick KL, eds. (1978). Alzheimer's Disease: Senile Dementia and Related Disorders. New York: Raven Press. p.595. ISBN978-0-89004-225-0.
↑Amaducci LA, Rocca WA, Schoenberg BS (November 1986). "Origin of the distinction between Alzheimer's disease and senile dementia: how history can clarify nosology". Neurology. 36 (11): 1497–1499. doi:10.1212/wnl.36.11.1497. PMID3531918. S2CID7689479.
↑Dubois B, Feldman HH, Jacova C, Dekosky ST, Barberger-Gateau P, Cummings J, etal. (August 2007). "Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria". The Lancet. Neurology. 6 (8): 734–746. doi:10.1016/S1474-4422(07)70178-3. PMID17616482. S2CID7356809.
↑Blacker D, Albert MS, Bassett SS, Go RC, Harrell LE, Folstein MF (December 1994). "Reliability and validity of NINCDS-ADRDA criteria for Alzheimer's disease. The National Institute of Mental Health Genetics Initiative". Archives of Neurology. 51 (12): 1198–1204. doi:10.1001/archneur.1994.00540240042014. PMID7986174.
↑Murray J, Schneider J, Banerjee S, Mann A (August 1999). "EUROCARE: a cross-national study of co-resident spouse carers for people with Alzheimer's disease: II—A qualitative analysis of the experience of caregiving". International Journal of Geriatric Psychiatry. 14 (8): 662–667. doi:10.1002/(SICI)1099-1166(199908)14:8<662::AID-GPS993>3.0.CO;2-4. PMID10489657. S2CID41741923.
↑Brodaty H, Hadzi-Pavlovic D (September 1990). "Psychosocial effects on carers of living with persons with dementia". The Australian and New Zealand Journal of Psychiatry. 24 (3): 351–361. doi:10.3109/00048679009077702. PMID2241719. S2CID11788466.
↑Pusey H, Richards D (May 2001). "A systematic review of the effectiveness of psychosocial interventions for carers of people with dementia". Aging & Mental Health. 5 (2): 107–119. doi:10.1080/13607860120038302. PMID11511058. S2CID32517015.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.