Opioid equivalency table
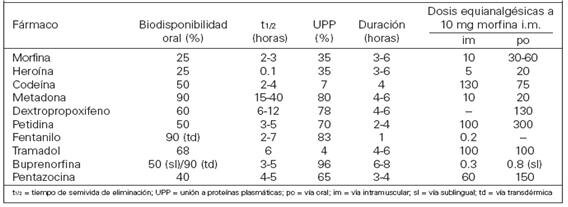
Opioids are a class of compounds that elicit analgesic (pain killing) effects in humans and animals by binding to the μ-opioid receptor within the central nervous system. The following table lists opioid and non-opioid analgesic drugs and their relative potencies. Values for the potencies represent opioids taken orally unless another route of administration is provided. As such, their bioavailabilities differ, and they may be more potent when taken intravenously. [9]
Nonlinearities
This chart measures pain relief versus mass of medication. Not all medications have a fixed relationship on this scale. Methadone is different from most opioids because its potency can vary depending on how long it is taken. Acute use (1–3 days) yields a potency about 1.5× stronger than that of morphine and chronic use (7 days+) yields a potency about 2.5 to 5× that of morphine. [10] [11] Similarly, the effect of tramadol increases after consecutive dosing due to the accumulation of its active metabolite and an increase of the oral bioavailability in chronic use. [12] [13]
Some of the data in this table has not been properly sourced and may well be unreliable. |
| Analgesic | Strength (relative) | Equivalent dose (10 mg oral morphine) [b] | Bioavailability | Half-life of active metabolites (hours) | Oral-to-parenteral ratio | Speed of onset | Duration | |
|---|---|---|---|---|---|---|---|---|
| Paracetamol [15] (non-opioid) | 1⁄360 | 3600 mg | 63–89% | 1–4 | 37 min (PO); 8 min (IV) | 5–6 hours | ||
| Aspirin [15] (NSAID, non-opioid) | 1⁄360 | 3600 mg | 80–100% | 3.1–9 | ||||
| Ibuprofen [15] (NSAID, non-opioid) | 1⁄222 | 2220 mg | 87–100% | 1.3–3 | ||||
| Diflunisal [15] (NSAID, non-opioid) | 1⁄160 | 1600 mg | 80–90% | 8–12 | ||||
| Naproxen [15] (NSAID, non-opioid) | 1⁄138 | 1380 mg | 95% | 12–24 | ||||
| Indomethacin [16] [17] (NSAID non-opioid) | 1⁄64 | |||||||
| Diclofenac [15] [18] (NSAID, non-opioid) | 1⁄10 | 100 mg (est.) | 50–60% | 1–4 | ||||
| Ketorolac [19] [20] (NSAID, non-opioid) | 1⁄3 | 30 mg IM (est.) [21] | 80–100% | 5–7 | ||||
| Nefopam [22] (Centrally-acting non-opioid) | 5⁄8 | 16 mg IM (est.) | Nefopam: 3–8, Desmethylnefopam 10–15 | |||||
| Piroxicam [23] [24] [25] (NSAID non-opioid) | 3 | 6.66 mg | 2–4 hours | 40 hours | ||||
| Dextropropoxyphene [26] | 1⁄20 | 130–200 mg | ||||||
| Codeine [27] | 1⁄10 [10] | 100–120 mg (PO) | ~90% | 2.5–3 (C6G 1.94; [28] morphine 2–3) | 15–30 min (PO) | 4–6 hours | ||
| Tramadol [27] | 1⁄10 | ~100 mg | 75% (IR), 85–90% (ER) | 6.0–8.8 [13] (M1) | ||||
| Opium [29] (oral) | 1⁄10 | ~100 mg | ~25% (morphine) | 2.5–3.0 (morphine, codeine) | ||||
| Tilidine [30] | 1⁄10 | 100 mg | 6% (parent drug), 99% (active metabolite) [31] | nortilidine 3.3 (PO) & 4.9 IV, bisnortilidine 5 (PO) & 6.9 (IV) [31] | 2.2:1 | 10–15 minutes (oral) 25–50 minutes (peak analgesic effect) | 3–4 hours | |
| Dihydrocodeine [32] [33] | 1⁄10 [10] | 100 mg | 20% | 4 | ||||
| Anileridine [34] | 1⁄4 | 40 mg | ||||||
| Alphaprodine [35] | 1⁄5 | 40–60 mg | ||||||
| Tapentadol [36] | 3⁄10 [10] | 32 mg | 32% (fasting) | |||||
| Pethidine (meperidine) [37] | 1⁄3 [10] | 30 mg SC/IV/IM 300 mg (PO) | 50–60% Orally, 100% SC/IV/IM | 3–5 | 5–15 sec if IV, 15–25 min if orally | |||
| Dipipanone [38] | 2⁄5 | 25 mg (PO) | 3.2–3.8 hours | ±4 hours | ||||
| Benzylfentanyl [39] [40] | 1⁄2 | |||||||
| AH-7921 [41] | 4⁄5 | |||||||
| SR-17018 [42] | 4⁄5 | 10–12 mg | 100% IV (Presumably) Unknown (researches are still being made) | 5–10 seconds if used IV and 15–25 min orally (PO) | ||||
| Nalbuphine [43] | 9⁄10 | 10–11 mg | ~33% (PO), 76% (SC), 81% (IM) [44] | 3–6 | 3 minutes, 10 minutes (peak effect) | 3–6 hours [45] | ||
| Hydrocodone [46] | 1 [10] | 10 mg | 70% [47] | 3.8–6 (Instant Release; PO) | 10–30 min (Instant Release; PO) | 4–6 | ||
| Pentazocine lactate (IV) [48] | 1 | 10 mg SC/IV/IM, 150 mg (PO) | ||||||
| Morphine (oral) | 1 | 10 mg | ~25% | 2–4 | 3:1 | 30 min (PO) | 3–6 hours | |
| Oxycodone (oral) [49] | 1.5 [10] | 6.67 mg | (60–87 / ±75% PO) / 78.2% [50] (IN) / 100% (IV/IM) or other parenteral administrations apart from spinal administration | 2–3 hours (Instant Release)(PO); 4.5 hours (Controlled Release)(PO) | 10–30 min (Instant Release)(PO); 1 hour (Controlled Release)(PO) | 3–6 hours (Instant Release)(PO); 10–12 hours (Controlled Release)(PO) [51] | ||
| Spiradoline [52] | 1.5–7.0 [53] | |||||||
| Nicomorphine [54] | 2–3 [55] | 3.33–5 mg | 20% | 4 | ||||
| Butorphanol [56] | 2.3 | 4.3 mg | ~12% (PO), 25–35% (SL), 70% (NAS) [57] | 3 (IM/IV) 4.5–5.5 (NAS) | 5.8:1 | 15 minutes | 3–4 hours | |
| Metopon [58] | 3 | 3.5 mg | ||||||
| Oxycodone (IV/IM) or other parenteral administrations apart from spinal administration [59] | 3–4 | 2.5–3.33 mg | (60–87 / ±75% PO) / 78.2% [50] (IN) / 100% (IV/IM) or other parenteral administrations apart from spinal administration | 1.5–3 (IV/IM) | 5 min (IV) [59] | 2–4 hours | ||
| Morphine [27] [60] (IV/IM) or other parenteral administrations apart from spinal administration | 3–4 | 2.5–3.33 mg | 100% | 3–4 | 3:1/4:1 | Instantaneously (from 5 to 15 sec; IV); 5–15 min (IM) | 3–7 hours | |
| Clonitazene [61] | 2–3 [62] | 3.33 mg | ||||||
| Methadone (acute) [63] [64] | 3–4 | 2.5–3.33 mg | 40–90% | 15–60 | 2:1 | |||
| Methadone (chronic) [64] | 2.5–5 [10] | 2–4 mg | 40–90% | 15–60 | 2:1 | |||
| Phenazocine [65] | 3.2–4.3 [66] | ~2.5 mg | 15 min (IV); 30 minutes (IM); 30–60 minutes (oral) [67] | 3–5 hours [68] | ||||
| Diamorphine (Heroin; IV/IM) or other parenteral administrations apart from spinal administration [69] | 4–5 (IV,IM) 2–2.5 (insufflated) [70] | 2–2.5 mg | 100% | <0.6 (morphine prodrug) [71] | Instantaneously (from 5 to 15 sec; IV); 2 to 5 min (IM) | 3 to 7 hours | ||
| 6-MAM [72] | 6–7 | 1.25–1.6 | 100% (IV,IM) | <0.6 (morphine prodrug) [71] | presumably 2:1 | Instantaneously (from 5 to 15 sec; IV); 2 to 5 min (IM) | 3 to 7 hours | |
| Dezocine [73] | 7.7–13 | 0.76–1.29 mg | 97% (IM) | 2.2 | 4–6 hours [74] | 5 min (IV); 5–15 min (IM/BUC); 6–8 hours (TD) [75] | ||
| Hydromorphone [76] [77] [36] | 10 (SC, IV, IM) 3–3.75 (PO) | 0.5–0.75 mg (SC, IV, IM) 2.5 mg (PO) [10] | Orally: 30–35%, Intranasal: 52–58%, IV/IM: 100% 62% | 2–3 | 5:1 | |||
| Oxymorphone [49] | 10 (SC, IV, IM) 3–4(PO) | 3.33 mg (PO), 0.333 mg (IV,IM & Interlaminar) | PO: 10% Buccal: 28% Sublingual: 37.5% Intranasal: 43% IV, IM & IT: 100% | 7.25–9.43 | 35 min (PO), Instantaneously (from 5 to 15 sec)(IV) | 6–8 hours orally 2–6 hours parenteral | ||
| U-47700 [78] | 7.5 | 1.5 mg | 1.5–3 | |||||
| Levorphanol [79] | 8 | 1.25 mg | 70% | 11–16 | 1:1 | |||
| Desomorphine [80] | 8–10 [81] | 1–1.25 mg | ~100% (IV) | 2–3 | Instantaneously (from 5 to 15 sec)(IV); 2–5 min (IM) | 3–4 hours | ||
| N-Phenethylnormorphine [82] | 8–14 | |||||||
| Alfentanyl [83] | 10–25 | 0.1–0.4 mg | 1.5 (90–111 minutes) | Instantaneously (from 5 to 15 sec); 4× more rapid than fentanyl | 0.25 hr (15 min); up to 54 minutes until offset of effects | |||
| Trefentanil [84] | 10 | |||||||
| Brifentanil [84] | 10–25 | |||||||
| Acetylfentanyl [84] | 15 [85] | |||||||
| 7-Hydroxymitragynine [86] | 17 | ~0.6 mg | ||||||
| Butyrfentanyl [87] | 25 | |||||||
| Enadoline [88] | 25 | 15 μg (threshold) and 0.160 mg/kg (dissociative effects) | ||||||
| Buprenorphine (SL) [26] | 40–80 [10] | 0.25 mg | 30% (SL); [89] ~100% (TD); 65% (BUC); [90] [91] 48% (INS) [92] | 20–70, mean 37 | 3:1 | 45 min | 12–24 hours | |
| N-Phenethyl-14-ethoxymetopon [82] | 60 | 160 μg | ||||||
| Furanylfentanyl [93] | 50–100 | |||||||
| Phenomorphan [94] | 60–80 | 0.13–0.16 mg | ||||||
| N-Phenethylnordesomorphine [95] | 85 | |||||||
| Phenaridine [96] | 50–100 | |||||||
| Fentanyl [27] | 50–100 [10] | 0.1 mg (100 μg) IM/IV | 33% (SL); 92% (TD); 89% (INS); 50% (BUC) | 0.04 (IV); 7 (TD) | 5 min (TD/IV) | 30–60 minutes (IV) | ||
| Metonitazene [97] | 100 | 0.1 mg/100 μg | ||||||
| Acrylfentanyl [84] | 50–100+ [98] | |||||||
| Remifentanil [99] | 100 | 100 μg | 100% (IM/IV) | 0.05 (3–6 min context-sensitive half-life; 7–18 min elimination half-life) [100] | Instantaneously (from 5 to 15 sec) | 15 minutes; rapid offset of effects necessitates continuous infusion for maintenance of anesthesia | ||
| Parafluorofentanyl (2-Fluorofentanyl) [101] | 111 | |||||||
| Buprenorphine (Transdermal) [102] [103] | 100–115 [10] | 0.1 mg (100 μg) | 30% (SL); [89] ~100% (TD); 65% (BUC); [90] [91] 48% (INS) [92] | 3:1 | 45–60 minutes | 12–24 hours | ||
| 14-Cinnamoyloxycodeinone [104] | 177 (median potency) 101–310 (varied potencies among test subjects) [104] | 77 μg | 2.8% (PO); 5.8% (SC) | 250:7 | ||||
| Protonitazepyne [97] | 190–200 [105] | 55–60 μg | ||||||
| Protonitazene [97] | 200 [106] | 50 μg | ||||||
| Ocfentanil [107] | 200 | 40–80 μg | ||||||
| Ro4-1539 [108] | 240–480 | 20–40 μg | ||||||
| 14-Methoxymetopon [109] | 500 (IV) | 20 μg | ||||||
| Isotonitazene [97] | 500 [110] | 20 μg | ||||||
| Sufentanil [27] | 500–1,000 [111] | 10–20 μg | 9% (PO); 52–59% (SL); 78% (BUC); 100% (IM/IV) [112] | 4.4 | 2:1 | 1–3 min (IV); 5 min (IN); 10 min (EPD); 6–15 min (SL) [113] | 30 min (IV); 40–50 min (SL) [114] [115] | |
| BDPC [116] | 504 | ~20 μg | ||||||
| Orthofluorofentanyl [101] | 564 | ~17 μg | ||||||
| C-8813 [116] | 591 | ~15 μg | ||||||
| 4-Phenylfentanyl [117] | 800 | |||||||
| Etonitazene [118] | 1,000–1,500 [119] | 6.6–10 μg | ||||||
| 3-Methylfentanyl [120] | 1,000 (3-methylfentanyl, (trans)-(+-)-isomer; 6,600 (3-methylfentanyl, (cis)-(-)-isomer) [121] | |||||||
| N-Desetylisotonitazene [122] [97] | 2,000 [123] | 5–10 μg | ||||||
| Etonitazepyne [105] [97] | 2,000 [124] | 5 μg | ||||||
| Etorphine [125] [126] | 500–2,000 [127] | 3.3–10 μg | ||||||
| Ohmefentanyl [128] | 6,300 [129] | |||||||
| Acetorphine [126] | 8,700 | 1.33 μg | ||||||
| Dihydroetorphine [130] | 12,000 | 0.83–10 μg (20–40 μg SL) | ||||||
| Carfentanil [131] | 10,000 | 1.0 μg | 7.7 | |||||
| Lofentanil [132] [133] | 10,000–11,000 [134] | |||||||
| 4-Carboethoxyohmefentanil [135] | 30,000 | |||||||
| Ohmecarfentanil [136] [135] | 30,000 | |||||||
| R-30490 [137] | 10,000–100,000 | |||||||
| 14-Methoxymetopon [138] | 1,000,000 (intrathecal & supraspinal) | 0.1 μg | ||||||
| PO: oral • BUC: buccal • SL: sublingual • TD: transdermal • IV: intravenous injection • IM: intramuscular injection • SC: subcutaneous injection • EPD: epidural injection "Strength" is defined as analgesic potency relative to oral morphine. Tolerance, sensitization, cross-tolerance, metabolism, and hyperalgesia may be complex factors in some individuals. Interactions with other drugs, food and drink, and other factors may increase or decrease the effect of certain analgesics and alter their half-life. Because some listed analgesics are prodrugs or have active metabolites, individual variation in liver enzymes (e.g., CYP2D6 enzyme) may result in significantly altered effects. | ||||||||
{kind=link}