
Pfizer Inc. is an American multinational pharmaceutical corporation. Pfizer is one of the world's largest pharmaceutical companies, and was ranked 64th on the 2020 Fortune 500 list of the largest U.S. corporations by total revenue, at $51.75 billion.

The Medicines and Healthcare products Regulatory Agency (MHRA) is an executive agency of the Department of Health and Social Care in the United Kingdom which is responsible for ensuring that medicines and medical devices work and are acceptably safe.
An Emergency Use Authorization (EUA) in the United States is an authorization granted to the Food and Drug Administration (FDA) under sections of the Federal Food, Drug, and Cosmetic Act as added to and amended by various Acts of Congress, including by the Pandemic and All-Hazards Preparedness Reauthorization Act of 2013 (PAHPRA) to allow the use of a drug prior to approval. It does not constitute approval of the drug in the full statutory meaning of the term, but instead authorizes FDA to facilitate availability of an unapproved product, or an unapproved use of an approved product, during a declared state of emergency from one of several agencies or of a "material threat" by the Secretary of Homeland Security.
Moderna is an American pharmaceutical and biotechnology company based in Cambridge, Massachusetts. It focuses on drug discovery, drug development, and vaccine technologies based exclusively on messenger RNA (mRNA).
An RNA vaccine or mRNA vaccine is a type of vaccine that uses a copy of a natural chemical called messenger RNA (mRNA) to produce an immune response. The vaccine transfects molecules of synthetic RNA into immunity cells. Once inside the immune cells, the vaccine's RNA functions as mRNA, causing the cells to build the foreign protein that would normally be produced by a pathogen or by a cancer cell. These protein molecules stimulate an adaptive immune response which teaches the body how to identify and destroy the corresponding pathogen or cancer cells. The delivery of mRNA is achieved by a co-formulation of the molecule into lipid nanoparticles which protect the RNA strands and helps their absorption into the cells.
A COVID‑19 vaccine is a vaccine intended to provide acquired immunity against COVID‑19. Prior to the COVID‑19 pandemic, work to develop a vaccine against coronavirus diseases like SARS and MERS established knowledge about the structure and function of coronaviruses; this knowledge enabled accelerated development of various vaccine technologies during early 2020.

Moderna COVID-19 Vaccine, codenamed mRNA-1273, is a COVID-19 vaccine developed by the United States National Institute of Allergy and Infectious Diseases (NIAID), the Biomedical Advanced Research and Development Authority (BARDA), and Moderna. It is administered by two 0.5 mL doses given by intramuscular injection given four weeks apart.
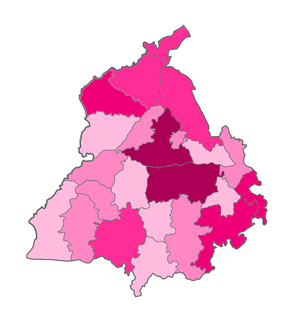
The COVID-19 pandemic was confirmed to have spread to the Indian state Punjab on 9 March 2020, when an Indian man returning from Italy was tested positive. As of 30 January 2021, the Ministry of Health and Family Welfare has confirmed a total of 173,084 cases, including 5,609 deaths and 165,291 recoveries in Punjab. The economy of Punjab has been severely effected by the COVID-19 pandemic.

AD5-nCOV, trade-named Convidicea, is a COVID-19 vaccine candidate being developed by Chinese biopharmaceutical company CanSino Biologics. Development of AD5-nCOV began in early 2020 and it entered Phase I testing in March and Phase II testing in April. Beginning in August 2020, it is in Phase III trials in Argentina, Chile, Mexico, Pakistan, Russia, and Saudi Arabia with estimated 40,500 participants using a single dose administration.

Operation Warp Speed (OWS) is a public–private partnership initiated by the U.S. government to facilitate and accelerate the development, manufacturing, and distribution of COVID-19 vaccines, therapeutics, and diagnostics. The first news report of Operation Warp Speed was on April 29, 2020, and the program was officially announced on May 15, 2020. It is headed by co-chair of the COVID-19 Advisory Board, David A. Kessler.

The Oxford–AstraZeneca COVID-19 vaccine, codenamed AZD1222, is a COVID-19 vaccine developed by Oxford University and AstraZeneca given by intramuscular injection, using as a vector the modified chimpanzee adenovirus ChAdOx1. One dosing regimen showed 90% efficacy when a half-dose was followed by a full-dose after at least one month, based on mixed trials with no participants over 55 years old. Another dosing regimen showed 62% efficacy when given as two full doses separated by at least one month.

BioNTech SE is a German biotechnology company based in Mainz that develops and manufactures active immunotherapies for patient-specific approaches to the treatment of diseases. It develops pharmaceutical candidates based on messenger ribonucleic acid (mRNA) for use as individualized cancer immunotherapies, as vaccines against infectious diseases and as protein replacement therapies for rare diseases, and also engineered cell therapy, novel antibodies and small molecule immunomodulators as treatment options for cancer.

The Pfizer–BioNTech COVID‑19 vaccine, sold under the brand name Comirnaty, is a COVID-19 vaccine developed by BioNTech in cooperation with Pfizer. It is both the first COVID-19 vaccine to be authorized by a stringent regulatory authority for emergency use and the first cleared for regular use.
BBIBP-CorV is one of two inactivated virus COVID-19 vaccines being developed by Sinopharm. As of December 2020, it is in Phase III trials in Argentina, Bahrain, Egypt, Morocco, Pakistan, Peru, and the United Arab Emirates (UAE) with over 60,000 participants. By November 2020, nearly one million people had taken the vaccine through China's emergency use program. By December 2020, almost 100,000 people in the UAE had also received the vaccine as part of a voluntary program.

BBV152 is an inactivated virus based COVID-19 vaccine being developed by Bharat Biotech in collaboration with the Indian Council of Medical Research.

The COVID-19 vaccination programme in the United Kingdom is the world's first mass immunisation campaign to protect against SARS-CoV-2 using vaccines developed in response to the COVID-19 pandemic.
The COVID-19 vaccination program in the Philippines will be an immunization campaign against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), in response to the ongoing pandemic in the country.

The COVID-19 vaccination campaign in Italy is a mass immunization campaign that was put in place by the Italian government in order to respond to the ongoing COVID-19 pandemic. It started on 27 December 2020, together with most countries in the European Union.
Ad26.COV2.S or JNJ-78436735 is a COVID-19 vaccine candidate developed by Janssen Vaccines and Beth Israel Deaconess Medical Center (BIDMC). It is a human adenovirus viral vector vaccine that requires only a single intramuscular injection. On January 29 2021, Janssen announced that it was 66% effective in a one-dose regimen.

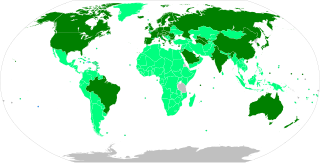
As of 29 January 2021, 90.44 million COVID‑19 vaccine doses had been administered worldwide based on official reports from national health agencies.





