The glucagon-like peptide-1 receptor (GLP1R) is a G protein-coupled receptor (GPCR) found on beta cells of the pancreas and on neurons of the brain. It is involved in the control of blood sugar level by enhancing insulin secretion. In humans it is synthesised by the geneGLP1R, which is present on chromosome 6.[5][6] It is a member of the glucagon receptor family of GPCRs.[7] GLP1R is composed of two domains, one extracellular (ECD) that binds the C-terminal helix of GLP-1,[8] and one transmembrane domain (TMD)[9] that binds the N-terminal region of GLP-1.[10][11][12] In the TMD domain a fulcrum of polar residues regulates the biased signaling of the receptor [10] while the transmembrane helical boundaries[13] and extracellular surface are a trigger for biased agonism.[11]
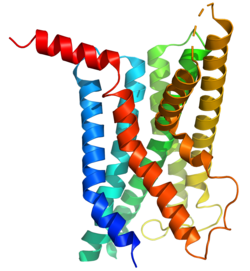
Structure of GLP1R-G protein complex bound to tirzepatide. Based on PDB entry 7RGP. Tirzepatide shown in red, GLP1R shown in green, G alpha subunit shown in white, G beta-gamma complex shown in dark gray.
The GLP-1 receptor is a transmembrane protein composed of seven alpha-helical transmembrane domains (TM1-TM7), an extracellular N-terminus, and an intracellular C-terminus. It belongs to the class B family of G protein-coupled receptors, also known as secretin-like receptors. The extracellular N-terminus contains key regions involved in ligand recognition and binding. It undergoes conformational changes upon ligand binding, leading to activation of intracellular signaling cascades. The intracellular C-terminus interacts with G proteins and other signaling molecules to initiate cellular responses.
Function
Glucagon-like peptide-1 (GLP-1) is a hormone consisting of 30 amino acids. GLP-1 is released by intestinal L cells when nutrients are consumed. GLP1R is expressed on beta cells in the pancreas. Binding of GLP-1 to GLP1R has multiple effects, including enhancing insulin secretion from pancreatic beta cells in response to glucose, increasing insulin expression, preventing beta-cell apoptosis, promoting the formation of new beta cells, reducing glucagon secretion, slowing down stomach emptying, promoting satiety, and improving glucose disposal in peripheral tissues.
GLP1R is also expressed in the brain[18] where it is involved in the control of appetite.[19]
Mechanism of action
Upon binding to its ligand GLP-1, the GLP-1 receptor activates intracellular signaling pathways that regulate insulin secretion, glucose metabolism, and satiety.
In pancreatic beta cells, GLP-1 receptor activation enhances glucose-stimulated insulin secretion. This occurs through the activation of adenylyl cyclase, leading to increased intracellular levels of cyclic AMP (cAMP). The rise in cAMP activates protein kinase A (PKA), which promotes insulin exocytosis and enhances beta cell survival and proliferation. GLP-1 receptor signaling in pancreatic alpha cells reduces glucagon secretion, further contributing to glucose lowering.
Activation of GLP-1 receptor delays the rate at which the stomach empties, leading to increased satiety and feeling of fullness.
Activation of the GLP-1 receptor in the brain promotes feelings of satiety.[19]
123456Maguire JJ, Davenport AP. "GLP-1 receptor". IUPHAR/BPS Guide to PHARMACOLOGY. International Union of Basic and Clinical Pharmacology. Retrieved 13 September 2015.
↑O'Brien A, Andrews S, Baig AH, Bortolato A, Brown JH, Brown GA, etal. (2019-08-09). "Identification of a novel allosteric GLP–1R antagonist HTL26119 using structure-based drug design". Bioorganic & Medicinal Chemistry Letters. 29 (20): 126611. doi:10.1016/j.bmcl.2019.08.015. PMID31447084. S2CID201749908.
Lankat-Buttgereit B, Göke R, Stöckmann F, Jiang J, Fehmann HC, Göke B (1994). "Detection of the human glucagon-like peptide 1(7-36) amide receptor on insulinoma-derived cell membranes". Digestion. 55 (1): 29–33. doi:10.1159/000201119. PMID8112494.
Graziano MP, Hey PJ, Borkowski D, Chicchi GG, Strader CD (October 1993). "Cloning and functional expression of a human glucagon-like peptide-1 receptor". Biochemical and Biophysical Research Communications. 196 (1): 141–6. Bibcode:1993BBRC..196..141G. doi:10.1006/bbrc.1993.2226. PMID8216285.
Stoffel M, Espinosa R, Le Beau MM, Bell GI (August 1993). "Human glucagon-like peptide-1 receptor gene. Localization to chromosome band 6p21 by fluorescence in situ hybridization and linkage of a highly polymorphic simple tandem repeat DNA polymorphism to other markers on chromosome 6". Diabetes. 42 (8): 1215–8. doi:10.2337/diabetes.42.8.1215. PMID8392011.
Dillon JS, Tanizawa Y, Wheeler MB, Leng XH, Ligon BB, Rabin DU, etal. (October 1993). "Cloning and functional expression of the human glucagon-like peptide-1 (GLP-1) receptor". Endocrinology. 133 (4): 1907–10. doi:10.1210/endo.133.4.8404634. PMID8404634.
Thorens B, Porret A, Bühler L, Deng SP, Morel P, Widmann C (November 1993). "Cloning and functional expression of the human islet GLP-1 receptor. Demonstration that exendin-4 is an agonist and exendin-(9-39) an antagonist of the receptor". Diabetes. 42 (11): 1678–82. doi:10.2337/diabetes.42.11.1678. PMID8405712.
Lankat-Buttgereit B, Göke B (1997). "Cloning and characterization of the 5' flanking sequences (promoter region) of the human GLP-1 receptor gene". Peptides. 18 (5): 617–24. doi:10.1016/S0196-9781(97)00001-6. PMID9213353. S2CID29733898.
Bazarsuren A, Grauschopf U, Wozny M, Reusch D, Hoffmann E, Schaefer W, etal. (May 2002). "In vitro folding, functional characterization, and disulfide pattern of the extracellular domain of human GLP-1 receptor". Biophysical Chemistry. 96 (2–3): 305–18. doi:10.1016/S0301-4622(02)00023-6. PMID12034449.
"Glucagon Receptor Family: GLP-1". IUPHAR Database of Receptors and Ion Channels. International Union of Basic and Clinical Pharmacology. Archived from the original on 2016-03-03. Retrieved 2007-10-25.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.